
Renal — MCQs

On this page
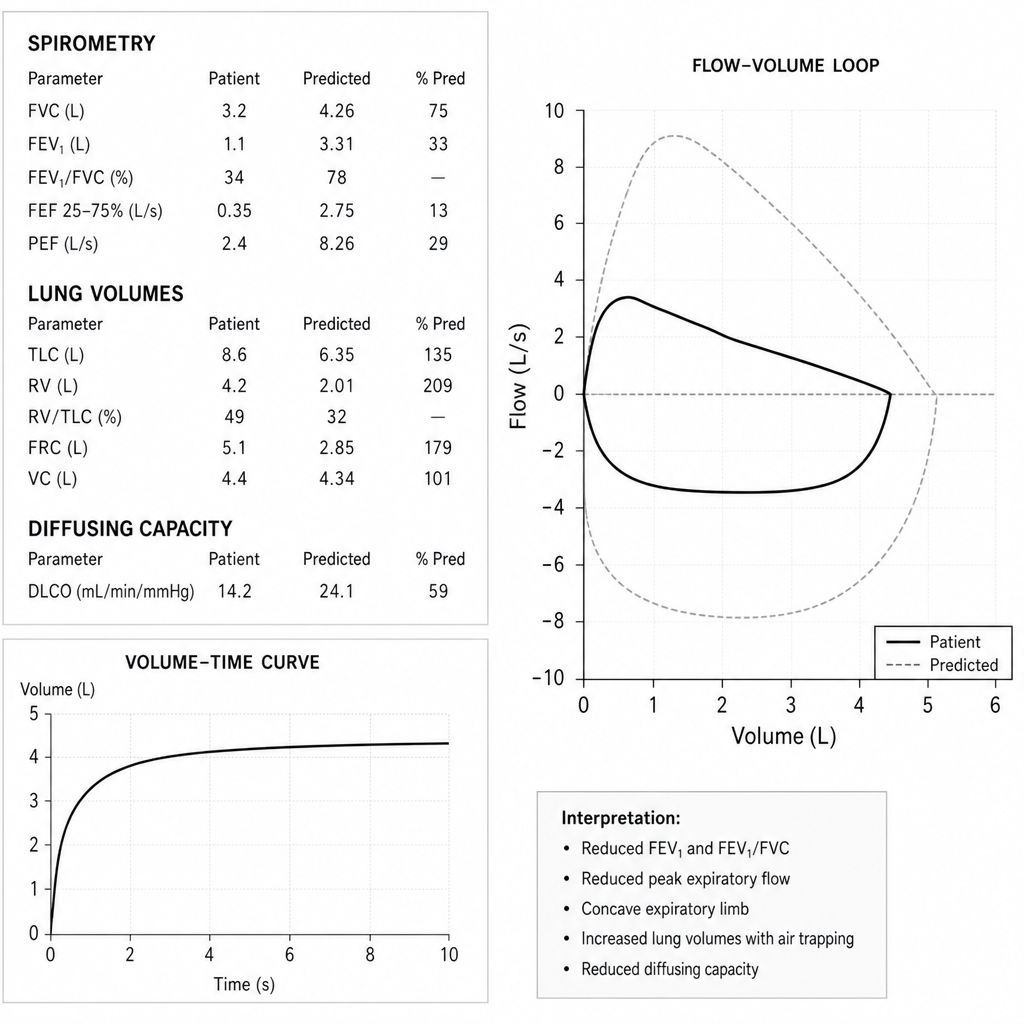
A 58-year-old man with chronic obstructive pulmonary disease is evaluated in the pulmonary function laboratory. Spirometry reveals an FEV1 of 1.1 L, FVC of 3.2 L, and a flow-volume loop. On the loop, peak expiratory flow is markedly reduced and the expiratory limb is concave toward the volume axis, while the inspiratory limb is normal in contour. Which of the following additional findings is most consistent with this pattern?
Renal clearance of substance Y is experimentally studied. At a constant glomerular filtration rate, it is found that the amount of substance Y excreted is greater than the amount filtered. This holds true across all physiologic values on the titration curve. Substance Y is most similar to which of the following?
A 30-year-old man presents to his physician for a follow-up appointment for a blood pressure of 140/90 mm Hg during his last visit. He was advised to record his blood pressure at home with an automated device twice every day. He recorded a wide range of blood pressure values in the past week, ranging from 110/70 mm Hg to 135/84 mm Hg. The medical history is unremarkable and he takes no medications. He occasionally drinks alcohol after work, but denies smoking and illicit drug use. Which of the following factors is responsible for maintaining a near-normal renal blood flow over a wide range of systemic blood pressures?
An investigator is studying bone metabolism and compares the serum studies and bone biopsy findings of a cohort of women 25–35 years of age with those from a cohort of women 55–65 years of age. Which of the following processes is most likely to be increased in the cohort of older women?
A 5-year-old boy is brought to the clinic for recurrent bedwetting. The child has an intellectual disability; thus, the mother is providing most of the history. She states that the child constantly drinks fluids and has a difficult time making it to the bathroom as often as he needs. Therefore, he sometimes wets himself during the day and at night. She has tried bedwetting alarms with no success. Review of systems is negative. His past medical history is unremarkable expect for moderate growth retardation. His temperature is 99.5°F (37.5°C), blood pressure is 80/54 mmHg, pulse is 90/min, respirations are 20/min, and oxygen saturation is 99% on room air. Routine laboratory tests and a 24 hour urine test are shown below. Serum: Na+: 138 mEq/L Cl-: 90 mEq/L K+: 2.5 mEq/L HCO3-: 35 mEq/L BUN: 9 mg/dL Glucose: 98 mg/dL Creatinine: 1.0 mg/dL Thyroid-stimulating hormone: 1.2 µU/mL Ca2+: 9.1 mg/dL AST: 13 U/L ALT: 10 U/L pH: 7.49 Urine: Epithelial cells: 5 cells Glucose: Negative WBC: 0/hpf Bacterial: None Protein: 60 mg/24h (Normal: < 150 mg/24h) Calcium: 370 mg/24h (Normal: 100-300 mg/24h) Osmolality 1600 mOsmol/kg H2O (Normal: 50-1400 mOsmol/kg H2O) What is the most likely explanation for this patient’s findings?
A 47-year-old man comes to the physician for a routine health maintenance examination. He states that he has felt fatigued and dizzy on several occasions over the past week. He has back pain for which he takes ibuprofen. Digital rectal examination shows no abnormalities. Laboratory studies show a hemoglobin concentration of 15 g/dL, a serum urea nitrogen concentration of 22 mg/dL, a serum creatinine concentration of 1.4 mg/dL, and a serum calcium concentration of 8.4 mg/dL. His prostate-specific antigen (PSA) level is 0.3 ng/mL (N < 4.5). An intravenous infusion of para-aminohippurate (PAH) is administered and its clearance is calculated. The patient's effective renal plasma flow is estimated to be 660 mL/min (N = 500–1350). The filtration fraction is calculated to be 9% (N = 17–23). Which of the following is the most likely cause of this patient's laboratory abnormalities?
A 9-year-old girl is being evaluated for suspected Bartter’s syndrome, a renal disorder caused by defective Cl- reabsorption by the Na+/K+/2Cl- cotransporter. In normal individuals, the segment of the nephron that houses this transporter is also characterized by which of the following?
A 32-year-old woman comes to her doctor’s office with abdominal distention, diffuse abdominal pain, and a history of 10–12 bowel movements a day for the last week. She was diagnosed with Crohn’s disease 3 years ago. Today, vitals are normal. Her abdomen is mildly distended and diffusely tender to palpation. A CT scan shows evidence of a fistula and strictures located in the last 30 cm of her ileum. A resection of the affected portion of the bowel is scheduled. What changes in bile metabolism are expected in this patient post-procedure?
A 35-year-old man is found in the wilderness behind a ski resort where he was lost for 2 days, and deprived of food and water. He is rushed to the emergency department for medical care. Which of the following parameters best describes his physiologic state when found?
A researcher needs to measure the volume of a specific body fluid compartment in subjects enrolled in his experiment. For such measurements, he injects an intravenous tracer into the subjects and then measures the concentration of the tracer in their blood samples. The volume of the specific body compartment will be calculated using the formula V = A/C, where V is the volume of the specific body fluid compartment, A is the amount of tracer injected, and C is the concentration of the tracer in the blood. For his experiment, he needs a tracer that is capillary membrane permeable but impermeable to cellular membranes. Which of the following tracers is most suitable for his experiment?
Practice by Chapter
Renal blood flow distribution
Practice Questions
Proximal tubule reabsorption
Practice Questions
Loop of Henle function
Practice Questions
Distal tubule and collecting duct function
Practice Questions
Concentration and dilution of urine
Practice Questions
Countercurrent multiplication system
Practice Questions
Sodium handling along the nephron
Practice Questions
Potassium balance and regulation
Practice Questions
Calcium and phosphate handling
Practice Questions
Magnesium handling
Practice Questions
Water balance and osmoregulation
Practice Questions
Diuretic mechanisms of action
Practice Questions
Integrated nephron function
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app