
Hemodynamics — MCQs

On this page
An experiment to determine the effects of gravity on blood pressure is conducted on 3 individuals of equal height and blood pressure oriented in different positions in space. Participant A is strapped in a supine position on a bed turned upside down in a vertical orientation with his head towards the floor and his feet towards the ceiling. Participant B is strapped in a supine position on a bed turned downwards in a vertical orientation with his head towards the ceiling and his feet just about touching the floor. Participant C is strapped in a supine position on a bed in a horizontal orientation. Blood pressure readings are then taken at the level of the head, heart, and feet from all 3 participants. Which of these positions will have the lowest recorded blood pressure reading?
A 73-year-old woman comes to the physician because of recurrent episodes of losing consciousness for several seconds upon standing. She has a history of hypertension, which has been treated with hydrochlorothiazide. Her blood pressure is 130/87 mm Hg in the supine position and 100/76 mm Hg 30 seconds after standing up. Cardiac examination shows no abnormalities. Which of the following sets of changes in venous return, cardiac output, and blood pressure (respectively) is most likely to occur when the patient stands up?
A 22-year-old man presents with a history of lightheadedness, weakness, and palpitations when he assumes an upright position from a supine position. He is otherwise a healthy man without a history of alcohol or other substance abuse. His supine and standing blood pressures (measured at 3-minute intervals) were 124/82 mm Hg and 102/72 mm Hg, respectively. He was advised to perform a Valsalva maneuver while monitoring blood pressure and heart rate to assess the integrity of his baroreflex control. Which of the following statements is correct?
During a clinical study evaluating the effects of exercise on muscle perfusion, 15 healthy individuals perform a 20-minute treadmill run at submaximal effort. Before and after the treadmill session, perfusion of the quadriceps muscle is evaluated with contrast-enhanced magnetic resonance imaging. The study shows a significant increase in muscle blood flow per unit of tissue mass. Which of the following local changes is most likely involved in the observed change in perfusion?
An 8-year-old boy is shifted to a post-surgical floor following neck surgery. The surgeon has restricted his oral intake for the next 24 hours. He does not have diarrhea, vomiting, or dehydration. His calculated fluid requirement is 1500 mL/day. However, he receives 2000 mL of intravenous isotonic fluids over 24 hours. Which of the following physiological parameters in the boy’s circulatory system is most likely to be increased?
A 71-year-old man is admitted to the hospital one hour after he was found unconscious. His pulse is 80/min and systolic blood pressure is 98 mm Hg; diastolic blood pressure cannot be measured. He is intubated and mechanically ventilated with supplemental oxygen at a tidal volume of 450 mL and a respiratory rate of 10/min. Arterial blood gas analysis shows: PCO2 43 mm Hg O2 saturation 94% O2 content 169 mL/L Pulmonary artery catheterization shows a pulmonary artery pressure of 15 mm Hg and a pulmonary capillary wedge pressure of 7 mm Hg. Bedside indirect calorimetry shows a rate of O2 tissue consumption of 325 mL/min. Given this information, which of the following additional values is sufficient to calculate the cardiac output in this patient?
A 32-year-old woman comes to the physician for a screening health examination that is required for scuba diving certification. The physician asks her to perform a breathing technique: following deep inspiration, she is instructed to forcefully exhale against a closed airway and contract her abdominal muscles while different cardiovascular parameters are evaluated. Which of the following effects is most likely after 10 seconds in this position?
A 40-year-old female volunteers for an invasive study to measure her cardiac function. She has no previous cardiovascular history and takes no medications. With the test subject at rest, the following data is collected using blood tests, intravascular probes, and a closed rebreathing circuit: Blood hemoglobin concentration 14 g/dL Arterial oxygen content 0.22 mL O2/mL Arterial oxygen saturation 98% Venous oxygen content 0.17 mL O2/mL Venous oxygen saturation 78% Oxygen consumption 250 mL/min The patient's pulse is 75/min, respiratory rate is 14/ min, and blood pressure is 125/70 mm Hg. What is the cardiac output of this volunteer?
A 66-year-old man is brought to the emergency department 20 minutes after being involved in a high-speed motor vehicle collision in which he was the unrestrained passenger. His wife confirms that he has hypertension, atrial fibrillation, and chronic lower back pain. Current medications include metoprolol, warfarin, hydrochlorothiazide, and oxycodone. On arrival, he is lethargic and confused. His pulse is 112/min, respirations are 10/min, and blood pressure is 172/78 mm Hg. The eyes open spontaneously. The pupils are equal and sluggish. He moves his extremities in response to commands. There is a 3-cm scalp laceration. There are multiple bruises over the right upper extremity. Cardiopulmonary examination shows no abnormalities. The abdomen is soft and nontender. Neurologic examination shows no focal findings. Two large-bore peripheral intravenous catheters are inserted. A 0.9% saline infusion is begun. A focused assessment with sonography in trauma is negative. Plain CT of the brain shows a 5-mm right subdural hematoma with no mass effect. Fresh frozen plasma is administered. Which of the following is most likely to reduce this patient's cerebral blood flow?
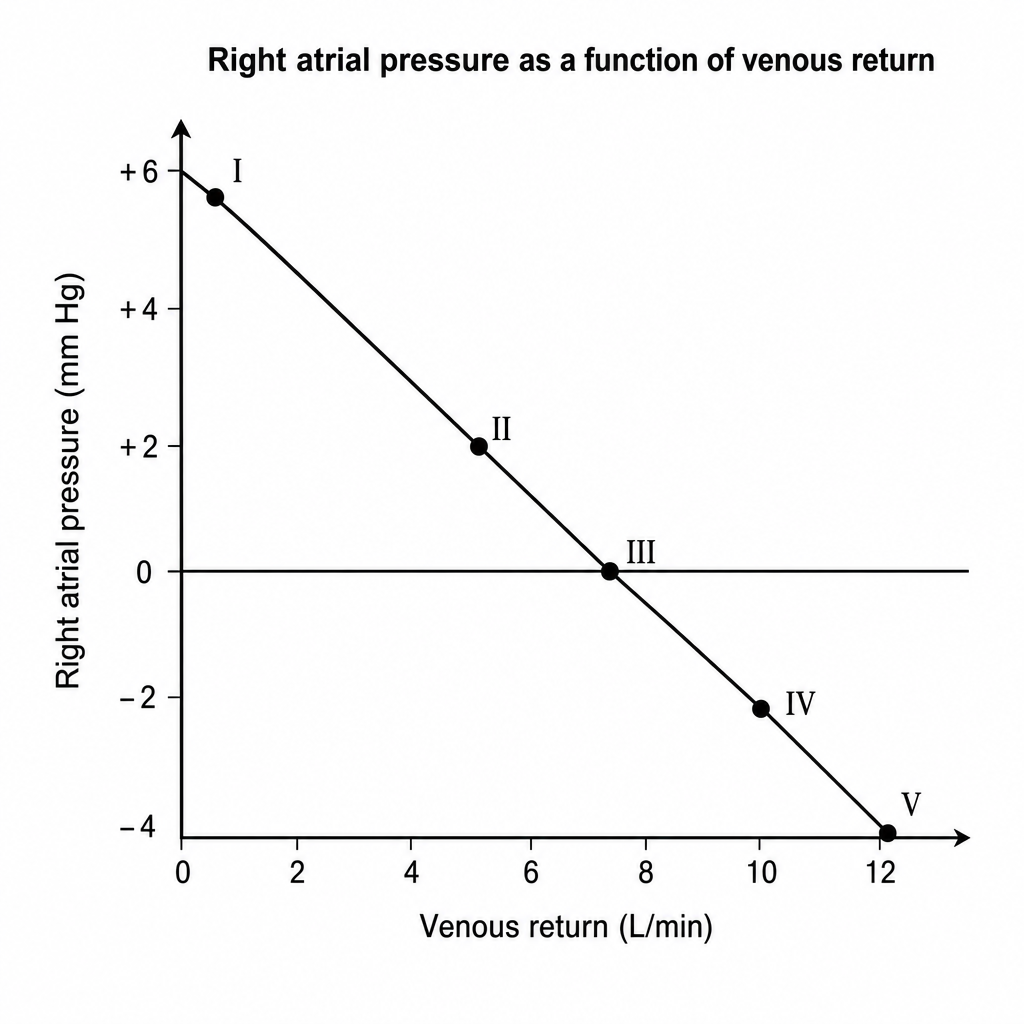
To study the flow of blood in the systemic circulation, partially occlusive stents are placed in the pulmonary trunk of a physiological system while the pressure in the right atrium is monitored. A graph where the right atrial pressure is a function of venous return is plotted. Assuming all circulatory nerve reflexes are absent in the system, at what point on the diagram shown below will the arterial pressure be closest to the venous pressure?
Practice by Chapter
Principles of blood flow (Poiseuille's law)
Practice Questions
Vascular resistance concepts
Practice Questions
Laminar vs. turbulent flow
Practice Questions
Pressure gradients across circulation
Practice Questions
Compliance of blood vessels
Practice Questions
Arterial pressure waveform
Practice Questions
Venous pressure and return
Practice Questions
Pulmonary circulation hemodynamics
Practice Questions
Autoregulation mechanisms
Practice Questions
Orthostatic changes in hemodynamics
Practice Questions
Shock states pathophysiology
Practice Questions
Hemodynamic monitoring principles
Practice Questions
Microcirculation physiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app