
Glomerular filtration — MCQs

On this page
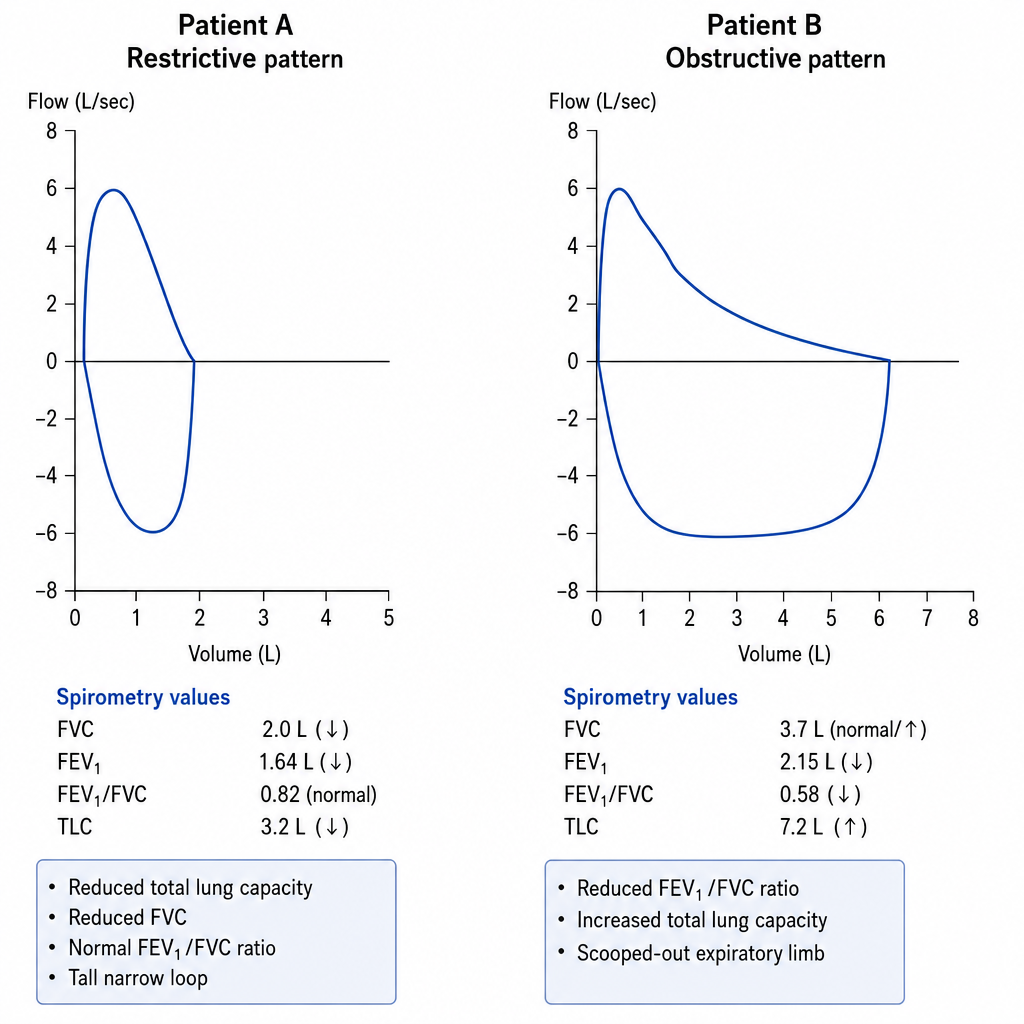
A pulmonologist reviews spirometry tracings from two patients with dyspnea. Patient A's loop demonstrates a reduced total lung capacity, reduced FVC, normal FEV1/FVC ratio (0.82), and a tall narrow loop. Patient B's loop shows a reduced FEV1/FVC ratio (0.58), increased total lung capacity, and a scooped-out expiratory limb. Which of the following correctly identifies the underlying mechanism responsible for the reduced expiratory flow in Patient B?
A 9-year-old boy is brought to the physician's office by his mother because of facial swelling for the past 2 days. The mother says that her son has always been healthy and active but is becoming increasingly lethargic and now has a puffy face. Upon inquiry, the boy describes a foamy appearance of his urine, but denies having blood in the urine, urinary frequency at night, or pain during urination. He has no history of renal or urinary diseases. Physical examination is unremarkable, except for generalized swelling of the face and pitting edema on the lower limbs. Dipstick analysis reveals 4+ proteinuria. An abdominal ultrasound shows normal kidney size and morphology. A renal biopsy yields no findings under light and fluorescence microscopy; however, glomerular podocyte foot effacement is noted on electron microscopy. Which of the following changes in Starling forces occurs in this patient's condition?
A 70-year-old female with chronic kidney failure secondary to diabetes asks her nephrologist to educate her about the techniques used to evaluate the degree of kidney failure progression. She learns about the concept of glomerular filtration rate (GFR) and learns that it can be estimated by measuring the levels of some substances. The clearance of which of the following substances is the most accurate estimate for GFR?
A 73-year-old male is brought in by ambulance after he was found to be lethargic and confused. He has not been routinely seeing a physician and is unable to recall how he came to be in the hospital. His temperature is 99°F (37°C), blood pressure is 150/95 mmHg, pulse is 75/min, and respirations are 18/min. His past medical history is significant for poorly controlled diabetes and longstanding hypertension, and he says that he has not been taking his medications recently. Labs are obtained and shown below: Serum: Na+: 142 mEq/L Cl-: 105 mEq/L K+: 5 mEq/L HCO3-: 16 mEq/L Urea nitrogen: 51 mg/dL Glucose: 224 mg/dL Creatinine: 2.6 mg/dL Which of the following changes would most likely improve the abnormal parameter that is responsible for this patient's symptoms?
A large pharmaceutical company is seeking healthy volunteers to participate in a drug trial. The drug is excreted in the urine, and the volunteers must agree to laboratory testing before enrolling in the trial. The laboratory results of one volunteer are shown below: Serum glucose (random) 148 mg/dL Sodium 140 mEq/L Potassium 4 mEq/L Chloride 100 mEq/L Serum creatinine 1 mg/dL Urinalysis test results: Glucose absent Sodium 35 mEq/L Potassium 10 mEq/L Chloride 45 mEq/L Creatinine 100 mg/dL Assuming a urine flow rate of 1 mL/min, which set of values below is the clearance of glucose, sodium, and creatinine in this patient?
An investigator is attempting to assess the glomerular filtration rate (GFR) of a healthy adult volunteer. The volunteer's inulin clearance is evaluated under continuous inulin infusion and urine collection and compared to the creatinine clearance. It is found that the estimated GFR based on the volunteer's creatinine clearance is 129 mL/min and the estimated GFR calculated using the inulin clearance is 122 mL/min. Which of the following is the best explanation for the difference in these measurements?
A researcher is studying the effects of a new antihypertensive medication on urine osmolality. She first measures urine osmolality in different parts of the nephron of a healthy human control. The findings are shown below: Portion of nephron Urine osmolality (mOsmol/kg) Proximal convoluted tubule 300 Loop of Henle, descending limb 1200 Loop of Henle, ascending limb 200 Distal convoluted tubule 100 Collecting duct 600 Which of the following is the most likely explanation for the urine osmolality in the ascending limb of the loop of Henle?
A 19-year-old man presents to the emergency department after a motor vehicle accident. The patient reports left shoulder pain that worsens with deep inspiration. Medical history is significant for a recent diagnosis of infectious mononucleosis. His temperature is 99°F (37.2°C), blood pressure is 80/55 mmHg, pulse is 115/min, and respiratory rate is 22/min. On physical exam, there is abdominal guarding, abdominal tenderness in the left upper quadrant, and rebound tenderness. The patient’s mucous membranes are dry and skin turgor is reduced. Which of the following most likely represents the acute changes in renal plasma flow (RPF) and glomerular filtration rate (GFR) in this patient?
To reduce the hemolysis that occurs with dialysis, researchers have developed an organic filtration membrane for dialysis that is believed to mimic the physiologic filtering apparatus of the human glomerulus. The permeability characteristics of this membrane are believed to be identical to those of the glomerular filtering membrane. Which of the following substances should be absent in the filtrate produced by this membrane?
A 55-year-old woman presents to a physician’s clinic for a diabetes follow-up. She recently lost weight and believes the diabetes is ‘winding down’ because the urinary frequency has slowed down compared to when her diabetes was "at its worst". She had been poorly compliant with medications, but she is now asking if she can decrease her medications as she feels like her diabetes is improving. Due to the decrease in urinary frequency, the physician is interested in interrogating her renal function. Which substance can be used to most accurately assess the glomerular filtration rate (GFR) in this patient?
Practice by Chapter
Glomerular structure and function
Practice Questions
Filtration barrier components
Practice Questions
Determinants of GFR
Practice Questions
Starling forces in glomerular filtration
Practice Questions
Renal blood flow autoregulation
Practice Questions
Filtration fraction
Practice Questions
GFR measurement methods
Practice Questions
Tubuloglomerular feedback
Practice Questions
Myogenic autoregulation
Practice Questions
Hormonal influences on GFR
Practice Questions
GFR in pathophysiological states
Practice Questions
Age-related changes in GFR
Practice Questions
Clinical estimation of GFR
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app