
Gas exchange — MCQs

On this page
A 23-year-old woman is brought to the emergency department by her friends because she thinks that she is having an allergic reaction. The patient is visibly distressed and insists on immediate attention as she feels like she is going to die. Her friends say they were discussing future plans while dining at a new seafood restaurant when her symptoms started. The patient has no history of allergies. She takes no medications and has no significant medical history. Her vitals include: pulse 98/min, respiratory rate 30/min, and blood pressure 120/80 mm Hg. On physical examination, she is tachypneic and in distress. Cardiopulmonary examination is unremarkable. No rash is seen on the body and examination of the lips and tongue reveals no findings. Which of the following would most likely present in this patient?
A 74-year-old woman presents with severe and progressively worsening shortness of breath. She says that her breathing has been difficult for many years but now it is troubling her a lot. She reports a 50-pack-year smoking history and drinks at least 2 alcoholic beverages daily. On physical examination, the patient is leaning forward in her seat and breathing with pursed lips. Which of the following mechanisms best explains the benefit of oxygen supplementation in this patient?
A 14-year-old boy is brought to the emergency department by his mom after she found him complaining of headaches, nausea, lightheadedness, and muscle pain. He has had type I diabetes for 3 years with very well managed blood sugars, and he is otherwise healthy. He recently returned from a boy scout skiing trip where he drank from a mountain stream, ate unusual foods, and lived in a lodge with a wood-fired fireplace and cooking stove. On physical exam he has a diffuse redness of his skin. Which of the following changes to this patient's pulmonary system would cause oxygen to exhibit similar tissue hypoxia effects as the most likely cause of this patient's symptoms?
A 60-year-old man presents with breathlessness for the past 3 months. His symptoms have been getting progressively worse during this time. He denies any history of cough, fever, or chest pain. He works at a local shipyard and is responsible for installing the plumbing aboard the vessels. His past medical history is significant for hypertension for which he takes metoprolol every day. He denies smoking and any illicit drug use. His pulse is 74/min, respiratory rate is 14/min, blood pressure is 130/76 mm Hg, and temperature is 36.8°C (98.2°F). Physical examination is significant for fine bibasilar crackles at the end of inspiration without digital clubbing. Which of the following additional findings would most likely be present in this patient?
A 25-year-old man is brought by his wife to the emergency department due to sudden onset confusion that started 40 minutes ago. The patient’s wife says that he came home from work complaining of pain in his arms and legs. While resting on the couch, he mentioned feeling nauseous and then became quite confused. He has no previous medical history and takes no medications. He does not smoke and only drinks alcohol occasionally. His vital signs include pulse 80/min, respiratory rate 12/min, blood pressure 120/84 mm Hg, and SaO2 99% on room air. On physical examination, the patient is oriented x 0 and unable to answer questions or follow commands. Generalized pallor is present. There are also multiple scratches on the face and neck due to constant itching. Assuming this patient’s symptoms are due to his employment, he most likely works as which of the following?
A 27-year-old man presents to the emergency department following a motor vehicle accident. Having been found as a restrained driver, he did not suffer from any chest injuries; nevertheless, his legs were pinned in position by the front of the highly damaged vehicle. After a prolonged extrication, the man sustained multiple fractures on his left femur and tibia. That same night, he underwent surgery to address his left leg fractures. In the next morning, the man suddenly developed severe dyspnea. Upon examination, he is noted to have a diffuse petechial rash. His vital signs are the following: blood pressure is 111/67 mm Hg, pulse rate is 107/min, respiratory rate is 27/min, oxygen saturation level is 82%, and his body temperature is normal. What is the most likely mechanism of his respiratory distress?
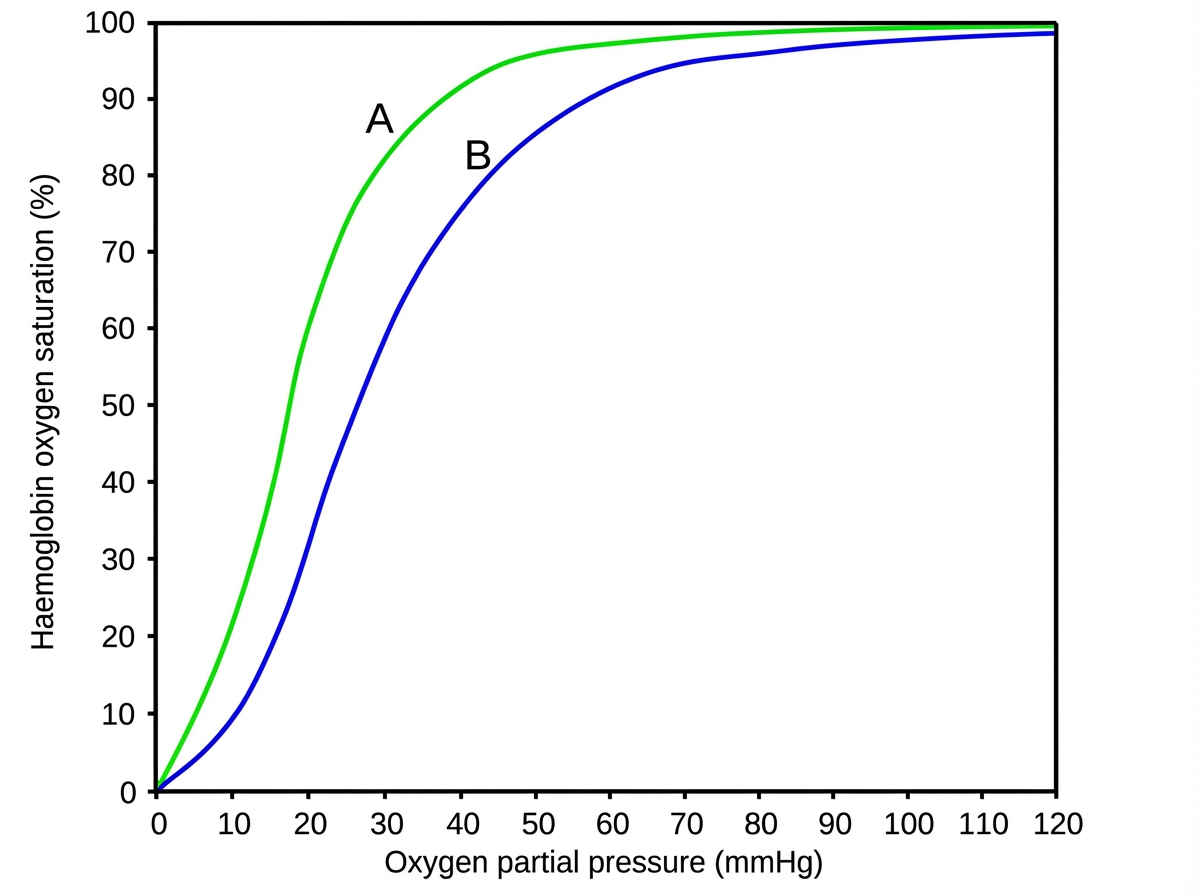
An investigator is studying the affinity of hemoglobin for oxygen in different clinical settings. An illustration of an oxygen-hemoglobin dissociation curve is shown. Curve A shows the test results of one of the research participants and curve B shows a normal oxygen-hemoglobin dissociation curve. Which of the following is most likely present in this research participant?
A 32-year-old female with Crohn's disease diagnosed in her early 20s comes to your office for a follow-up appointment. She is complaining of headaches and fatigue. Which of the following arterial blood gas findings might you expect?
A research scientist attempts to understand the influence of carbon dioxide content in blood on its oxygen binding. The scientist adds carbon dioxide to dog blood and measures the uptake of oxygen in the blood versus oxygen pressure in the peripheral tissue. He notes in one dog that with the addition of carbon dioxide with a pressure of 90 mmHg, the oxygen pressure in the peripheral tissue rose from 26 to 33 mmHg. How can this phenomenon be explained?
Practice by Chapter
Oxygen transport in blood
Practice Questions
Hemoglobin-oxygen binding
Practice Questions
Oxygen-hemoglobin dissociation curve
Practice Questions
Bohr effect and rightward shifts
Practice Questions
2,3-DPG effects on oxygen affinity
Practice Questions
Carbon dioxide transport
Practice Questions
Chloride shift mechanism
Practice Questions
Ventilation-perfusion matching
Practice Questions
Diffusion limitation vs perfusion limitation
Practice Questions
Alveolar-arterial oxygen gradient
Practice Questions
Hypoxemia mechanisms
Practice Questions
Altitude physiology
Practice Questions
Diving physiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app