
ECG interpretation — MCQs

On this page
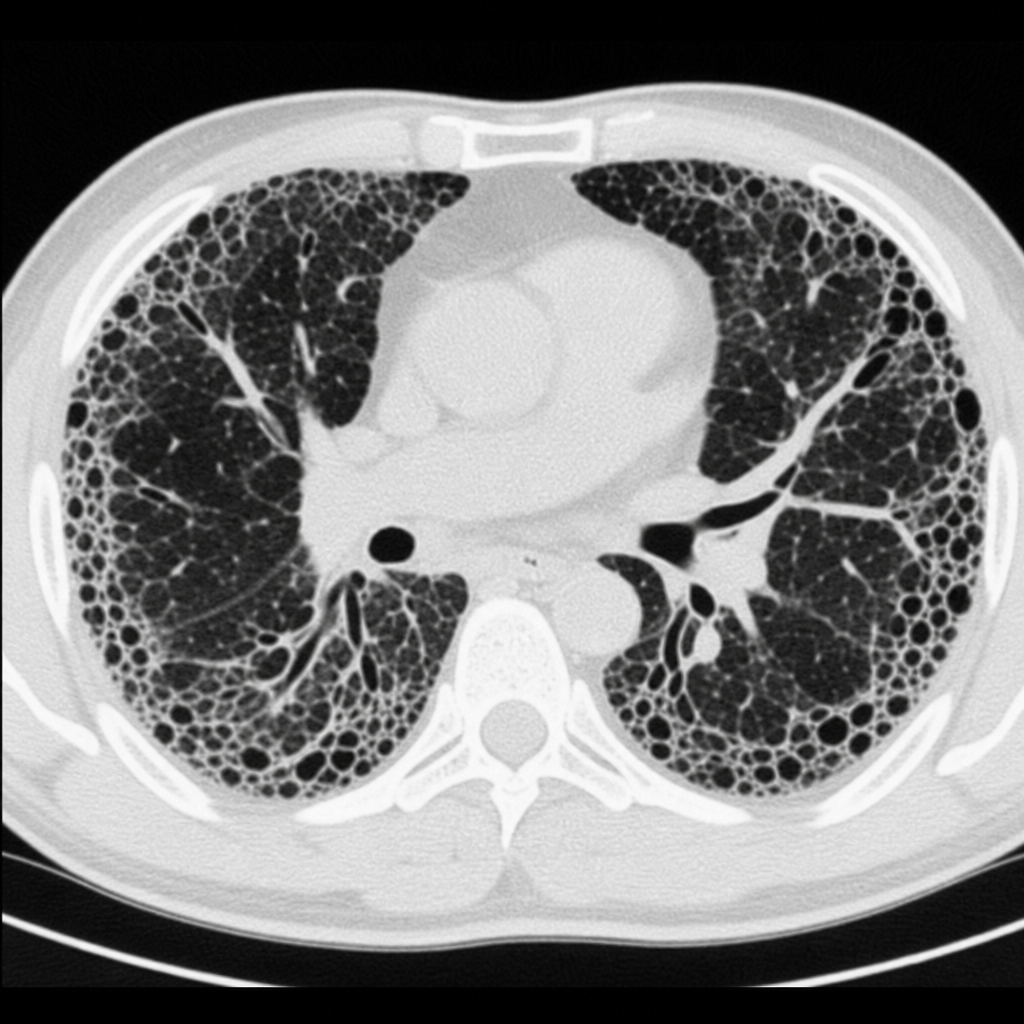
A 19-year-old male college student presents with progressive exertional dyspnea over 6 months. He has a history of childhood radiation therapy to the chest for mediastinal lymphoma. High-resolution CT of the chest shows bilateral interstitial fibrosis with honeycombing and traction bronchiectasis. Pulmonary function testing yields the following results: FVC 3.1 L (predicted 4.8 L), FEV1 2.7 L (predicted 4.0 L), FEV1/FVC 87%, TLC 3.4 L (predicted 6.2 L), DLCO 58% of predicted. Which of the following physiological mechanisms best accounts for the reduced DLCO in this patient?
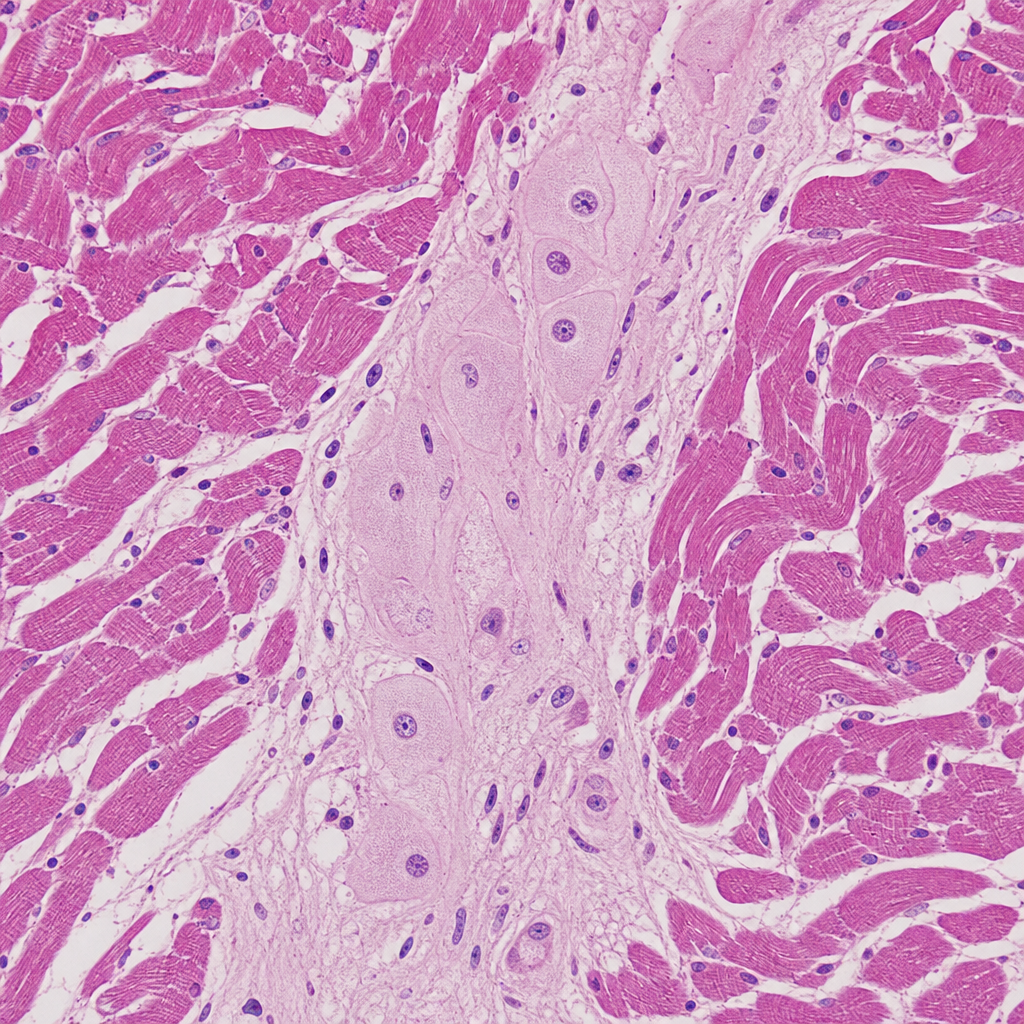
An investigator develops a new drug that decreases the number of voltage-gated potassium channels in cardiac muscle cell membranes. Which of the following is the most likely effect of this drug on the myocardial action potential?
A 17-year-old girl suddenly grabs her chest and collapses to the ground while playing volleyball at school. The teacher rushes to evaluate the situation and finds that the girl has no pulse and is not breathing. He starts chest compressions. An automated external defibrillator (AED) is brought to the scene within 3 minutes and a shock is delivered. The girl regains consciousness and regular sinus rhythm. She is rushed to the emergency department. The vital signs include: blood pressure 122/77 mm Hg and pulse 65/min. The pulse is regular. An electrocardiogram (ECG) shows a shortened PR interval, a wide QRS complex, a delta wave, and an inverted T wave. Which of the following is the most likely pathology in the conduction system of this patient’s heart?
A 55-year-old man presents to his physician with weakness and fatigue for 1 week. There is no significant past medical history. He mentions that he is very health conscious and has heard about the health benefits of juices. He is following a juice-only diet for the last 2 weeks. His physical examination is completely normal, except for depressed deep tendon reflexes. The only abnormality in a complete laboratory evaluation is a serum potassium level of 6.0 mEq/L (6.0 mmol/L). There are significantly peaked T-waves on ECG. Which of the following pathophysiologic mechanisms best explains the patient’s symptoms?
A researcher is studying how electrical activity propagates across the heart. In order to do this, he decides to measure the rate at which an action potential moves within various groups of cardiac muscle tissue. In particular, he isolates fibers from areas of the heart with the following characteristics: A) Dysfunction leads to fixed PR intervals prior to a dropped beat B) Dysfunction leads to increasing PR intervals prior to a dropped beat C) Dysfunction leads to tachycardia with a dramatically widened QRS complex D) Dysfunction leads to tachycardia with a sawtooth pattern on electrocardiogram Which of the following is the proper order of these tissues from fastest action potential propagation to slowest action potential propagation.
A cardiologist is studying how a new virus that infects the heart affects the electrical conduction system of the cardiac myocytes. He decides to obtain electrocardiograms on patients with this disease in order to see how the wave patterns and durations change over time. While studying these records, he asks a medical student who is working with him to interpret the traces. Specifically, he asks her to identify the part that represents initial ventricular depolarization. Which of the following characteristics is most consistent with this feature of the electrocardiogram?
A 50-year-old woman presents to the emergency department with mild chest pressure that does not radiate to her left arm or jaw. These episodes have been ongoing several times over the last 24 hours. Her medical history is significant for diabetes mellitus type II and HTN for which she takes metformin and lisinopril. Her physical exam is significant for a middle aged woman appearing as stated age in moderate distress. Her heart and lung sounds are within normal limits. On laboratory examination, her troponin level is elevated, and her heart rate waivers around 47/min. Note this patient’s EKG in the exhibit. Which pacemaker site is likely in use in this patient?
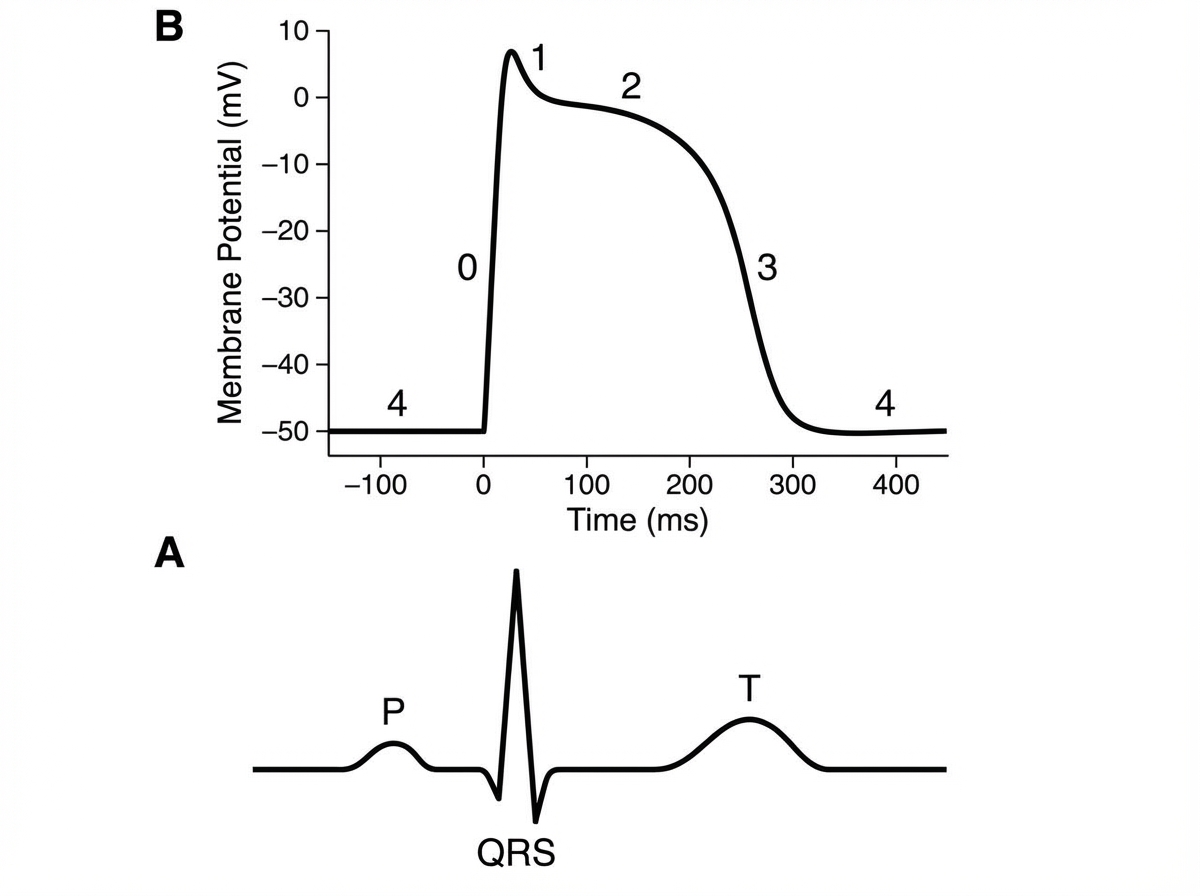
A 48-year-old female comes into the ER with chest pain. An electrocardiogram (EKG) shows a heart beat of this individual in Image A. The QRS complex best correlates with what part of the action potential of the ventricular myocyte shown in Image B?
A 65-year-old woman comes to the physician because of a 3-month history of intermittent palpitations and shortness of breath. Cardiopulmonary examination shows no other abnormalities. An ECG shows an absence of P waves, an oscillating baseline, and irregular RR intervals at a rate of approximately 95 beats per minute. The difference between atrial and ventricular rates in this patient is most likely due to which of the following?
A 42-year-old Caucasian woman is enrolled in a randomized controlled trial to study cardiac function in the setting of several different drugs. She is started on verapamil and instructed to exercise at 50% of her VO2 max while several cardiac parameters are being measured. During this experiment, which of the following represents the relative conduction speed through the heart from fastest to slowest?
Practice by Chapter
ECG basics and lead placement
Practice Questions
Cardiac axis determination
Practice Questions
P wave and atrial depolarization
Practice Questions
PR interval significance
Practice Questions
QRS complex analysis
Practice Questions
ST segment evaluation
Practice Questions
T wave and repolarization
Practice Questions
QT interval and QTc calculation
Practice Questions
Bundle branch blocks
Practice Questions
Chamber enlargement patterns
Practice Questions
Ischemia and infarction patterns
Practice Questions
Common arrhythmia recognition
Practice Questions
Electrolyte effects on ECG
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app