
Compliance — MCQs

On this page
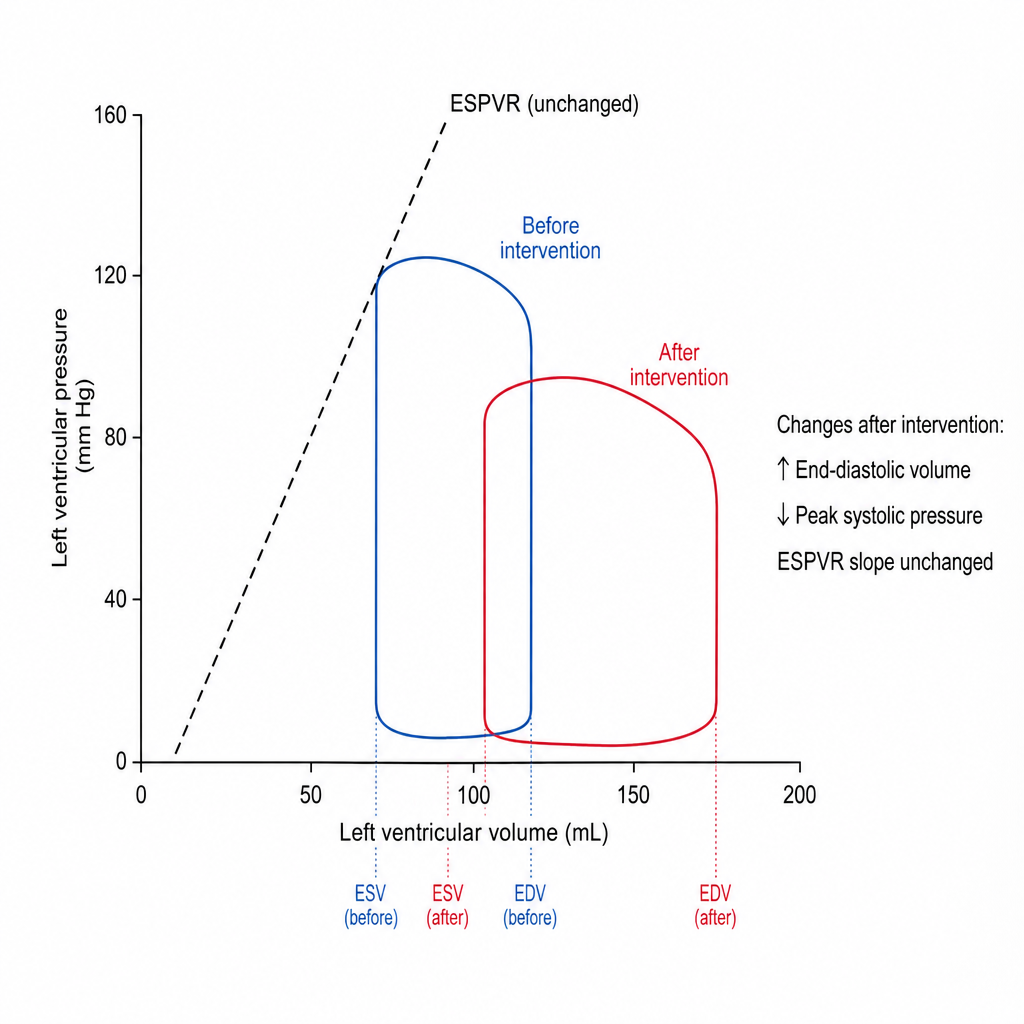
A pressure-volume loop is recorded from the left ventricle of a patient before and after an intervention. The post-intervention loop is shifted rightward with a larger end-diastolic volume, a lower peak systolic pressure, and the slope of the end-systolic pressure-volume relationship (ESPVR) is unchanged. Which of the following interventions most likely produced this change?
Practice by Chapter
Definition of lung compliance
Practice Questions
Static vs dynamic compliance
Practice Questions
Pressure-volume curves
Practice Questions
Surfactant function and synthesis
Practice Questions
Surface tension effects on compliance
Practice Questions
Elastic recoil of lung tissue
Practice Questions
Chest wall compliance
Practice Questions
Combined respiratory system compliance
Practice Questions
Altered compliance in disease states
Practice Questions
Restrictive lung disease mechanics
Practice Questions
Obstructive lung disease effects
Practice Questions
Compliance measurement techniques
Practice Questions
Age-related changes in compliance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app