
Cardiovascular — MCQs

On this page
A 28-year-old man presents to his primary care physician for a general checkup. The patient is a healthy young man with no significant past medical history. He is a MD/PhD student and lives in New York City. He exercises frequently and is doing very well in school. He is currently sexually active with multiple female partners and does not use protection. His temperature is 98.9°F (37.2°C), blood pressure is 147/98 mmHg, pulse is 90/min, respirations are 14/min, and oxygen saturation is 99% on room air. Physical exam is notable for a very muscular young man. The patient has comedonal acne and palpable breast tissue. Testicular exam reveals small and symmetrical testicles. Which of the following laboratory changes is most likely to be found in this patient?
An 11-year-old boy presents with a 2-day history of uncontrollable shivering. During admission, the patient’s vital signs are within normal limits, except for a fluctuating body temperature registering as low as 35.0°C (95.0°F) and as high as 40.0°C (104.0°F), requiring alternating use of cooling and warming blankets. A complete blood count (CBC) is normal, and a chest radiograph is negative for consolidations and infiltrates. An MRI of the brain reveals a space-occupying lesion infiltrating the posterior hypothalamus and extending laterally. Which of the following additional findings are most likely, based on this patient’s physical examination?
A 25-year-old woman presents to her primary care physician for her yearly physical exam. She has no past medical history and says that she does not currently have any health concerns. On physical exam, she is found to have hyperactive patellar reflexes but says that she has had this finding since she was a child. She asks her physician why this might be the case. Her physician explains that there are certain cells that are responsible for detecting muscle stretch and responding to restore the length of the muscle. Which of the following is most likely a characteristic of these structures?
A 71-year-old man comes to the physician because of decreased sexual performance for the past 2 years. He reports that it takes longer for his penis to become erect, and he cannot maintain an erection for as long as before. His ejaculations have become less forceful. Once he has achieved an orgasm, he requires several hours before he can have another orgasm. He has been happily married for 40 years and he has no marital conflicts. His only medication is esomeprazole for gastroesophageal reflux disease. Examination shows coarse dark pubic and axillary hair. The skin of his lower extremity is warm to the touch; pedal pulses and sensation are intact. Rectal examination shows a symmetrically enlarged prostate with no masses. His fasting serum glucose is 96 mg/dL and his prostate-specific antigen is 3.9 ng/mL (N < 4). Which of the following etiologies is the most likely cause of the patient's symptoms?
A 56-year-old woman presents to the emergency department with an episode of nausea and severe unrelenting right upper abdominal pain. She had a cholecystectomy for gallstones a year earlier and has since experienced frequent recurrences of abdominal pain, most often after a meal. Her past medical history is otherwise unremarkable and she only takes medications for her pain when it becomes intolerable. Her physical exam is normal except for an intense abdominal pain upon deep palpation of her right upper quadrant. Her laboratory values are unremarkable with the exception of a mildly elevated alkaline phosphatase, amylase, and lipase. Her abdominal ultrasound shows a slightly enlarged common bile duct at 8 mm in diameter (N = up to 6 mm) and a normal pancreatic duct. The patient is referred to a gastroenterology service for an ERCP (endoscopic retrograde cholangiopancreatography) to stent her common bile duct. During the procedure the sphincter at the entrance to the duct is constricted. Which statement best describes the regulation of the function of the sphincter which is hampering the cannulation of the pancreatic duct in this patient?
A 34-year-old woman comes to the physician because she has not had her period for 4 months. Menses had previously occurred at regular 28-day intervals with moderate flow. A home pregnancy test was negative. She also reports recurrent headaches and has noticed that when she goes to the movies she cannot see the outer edges of the screen without turning her head to each side. This patient's symptoms are most likely caused by abnormal growth of which of the following?
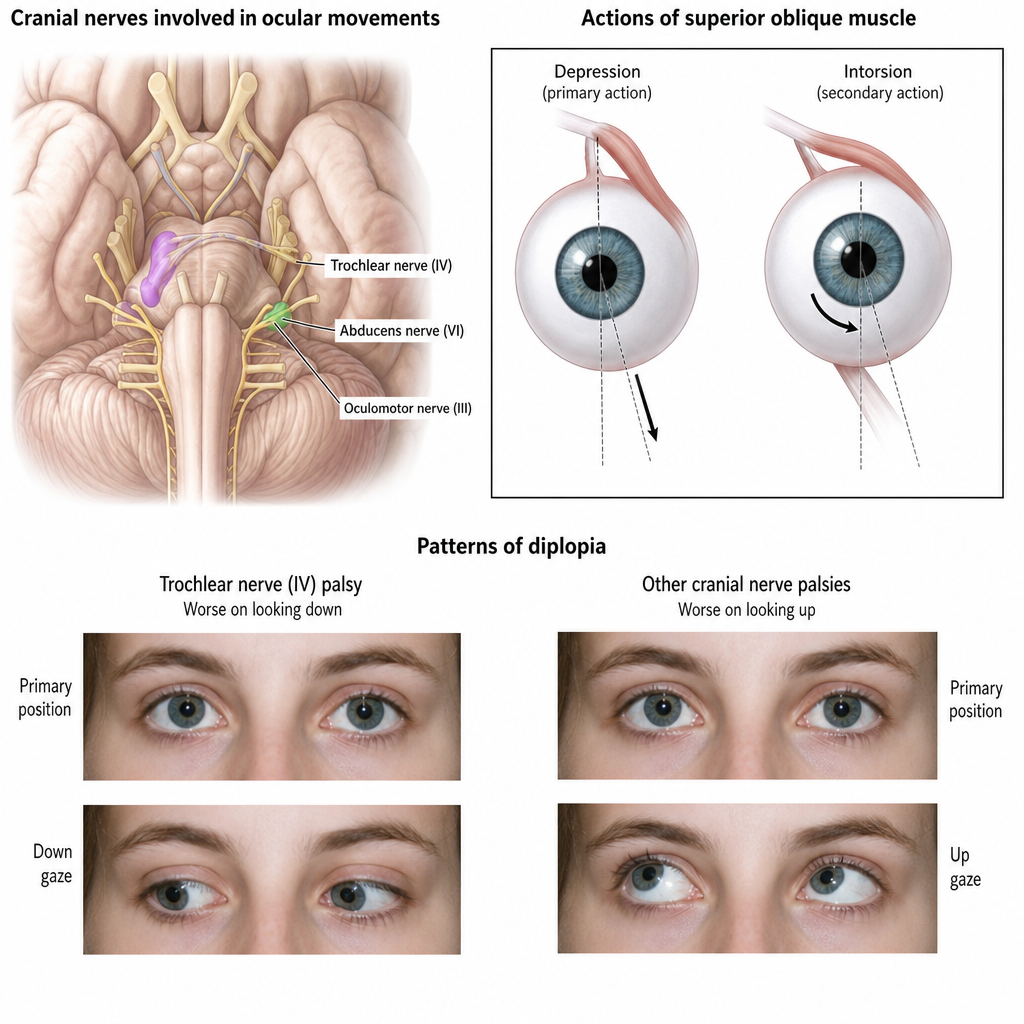
A 9-year-old girl is brought to the emergency department with a headache and double vision 1 hour after being hit on the head while playing with a friend. Her friend's elbow struck her head, just above her left ear. She did not lose consciousness, but her mother reports that she was confused for 20 minutes after the incident and did not recall being hit. She appears healthy. She is alert and oriented to person, place, and time. Her temperature is 37.2°C (99°F), pulse is 86/min, respirations are 15/min, and blood pressure is 118/78 mmHg. Examination shows the head tilted toward the right shoulder. A photograph of the eyes at primary gaze is shown. There is mild tenderness to palpation over the left temporal bone. Visual acuity is 20/20 in both eyes when tested independently. The patient's left eye hypertropia worsens with right gaze and when the patient tilts her head toward her left shoulder. The pupils are equal and reactive to light. Muscle strength and sensation are intact bilaterally. Deep tendon reflexes are 2+ bilaterally. Plantar reflex shows a flexor response. Which of the following is the most likely cause of this patient's ocular symptoms?
A 60-year-old male engineer who complains of shortness of breath when walking a few blocks undergoes a cardiac stress test because of concern for coronary artery disease. During the test he asks his cardiologist about what variables are usually used to quantify the functioning of the heart. He learns that one of these variables is stroke volume. Which of the following scenarios would be most likely to lead to a decrease in stroke volume?
A 25-year-old man is admitted to the hospital after a severe motor vehicle accident as an unrestrained front-seat passenger. Appropriate life-saving measures are given, and the patient is now hemodynamically stable. Physical examination shows a complete loss of consciousness. There are no motor or ocular movements with painful stimuli. The patient has bilaterally intact pupillary light reflexes. The patient is placed in a 30° semi-recumbent position for further examination. What is the most likely finding on the examination of this patient's right ear?
A 38-year-old woman presents to the physician’s clinic with a 6-month history of generalized weakness that usually worsens as the day progresses. She also complains of the drooping of her eyelids and double vision that is worse in the evening. Physical examination reveals bilateral ptosis after a sustained upward gaze and loss of eye convergence which improves upon placing ice packs over the eyes and after the administration of edrophonium. Which of the following is an intrinsic property of the muscle group affected in this patient?
Practice by Chapter
Cardiac output determinants
Practice Questions
Starling's law of the heart
Practice Questions
Preload and afterload concepts
Practice Questions
Contractility determinants
Practice Questions
Regulation of blood pressure
Practice Questions
Baroreceptor reflexes
Practice Questions
Neural control of cardiovascular function
Practice Questions
Endothelial function and dysfunction
Practice Questions
Coronary blood flow regulation
Practice Questions
Regional blood flow distribution
Practice Questions
Exercise cardiovascular physiology
Practice Questions
Aging effects on cardiovascular system
Practice Questions
Integrated cardiovascular responses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app