
Cardiovascular — MCQs

On this page
A neurophysiology expert is teaching his students the physiology of the neuromuscular junction. While describing the sequence of events that takes place at the neuromuscular junction, he mentions that as the action potential travels down the motor neuron, it causes depolarization of the presynaptic membrane. This results in the opening of voltage-gated calcium channels, which leads to an influx of calcium into the synapse of the motor neuron. Consequently, the cytosolic concentration of Ca2+ ions increases. Which of the following occurs at the neuromuscular junction as a result of this increase in cytosolic Ca2+?
An investigator is studying muscle contraction in tissue obtained from the thigh muscle of an experimental animal. After injection of radiolabeled ATP, the tissue is stimulated with electrical impulses. Radioassay of these muscle cells is most likely to show greatest activity in which of the following structures?
A 40-year-old Caucasian male presents to the emergency room after being shot in the arm in a hunting accident. His shirt is soaked through with blood. He has a blood pressure of 65/40, a heart rate of 122, and his skin is pale, cool to the touch, and moist. This patient is most likely experiencing all of the following EXCEPT:
A 56-year-old woman is admitted to the hospital for progressive bilateral lower extremity weakness and absent deep tendon reflexes. Cerebrospinal fluid analysis shows an elevated protein concentration and a normal cell count. Treatment with plasmapheresis is initiated, after which her symptoms start to improve. Four weeks after her initial presentation, physical examination shows normal muscle strength in the bilateral lower extremities and 2+ deep tendon reflexes. Which of the following changes in neuronal properties is the most likely explanation for the improvement in her neurological examination?
A 45-year-old man comes to the physician because of persistent reddening of the face for the past 3 months. During this period he also had difficulty concentrating at work and experienced generalized fatigue. He has fallen asleep multiple times during important meetings. His mother has rheumatoid arthritis. He has hypertension and asthma. He has smoked one pack of cigarettes daily for 28 years and drinks one alcoholic beverage per day. Medications include labetalol and a salbutamol inhaler. He is 170 cm (5 ft 7 in) tall and weighs 88 kg (194 lb); BMI is 30.4 kg/m2. His temperature is 37.1°C (98.8°F), pulse is 88/min, respirations are 14/min, and blood pressure is 145/85 mm Hg. Physical examination shows erythema of the face that is especially pronounced around the cheeks, nose, and ears. His neck appears short and wide. The remainder of the examination shows no abnormalities. Which of the following is the most likely cause of this patient's facial discoloration?
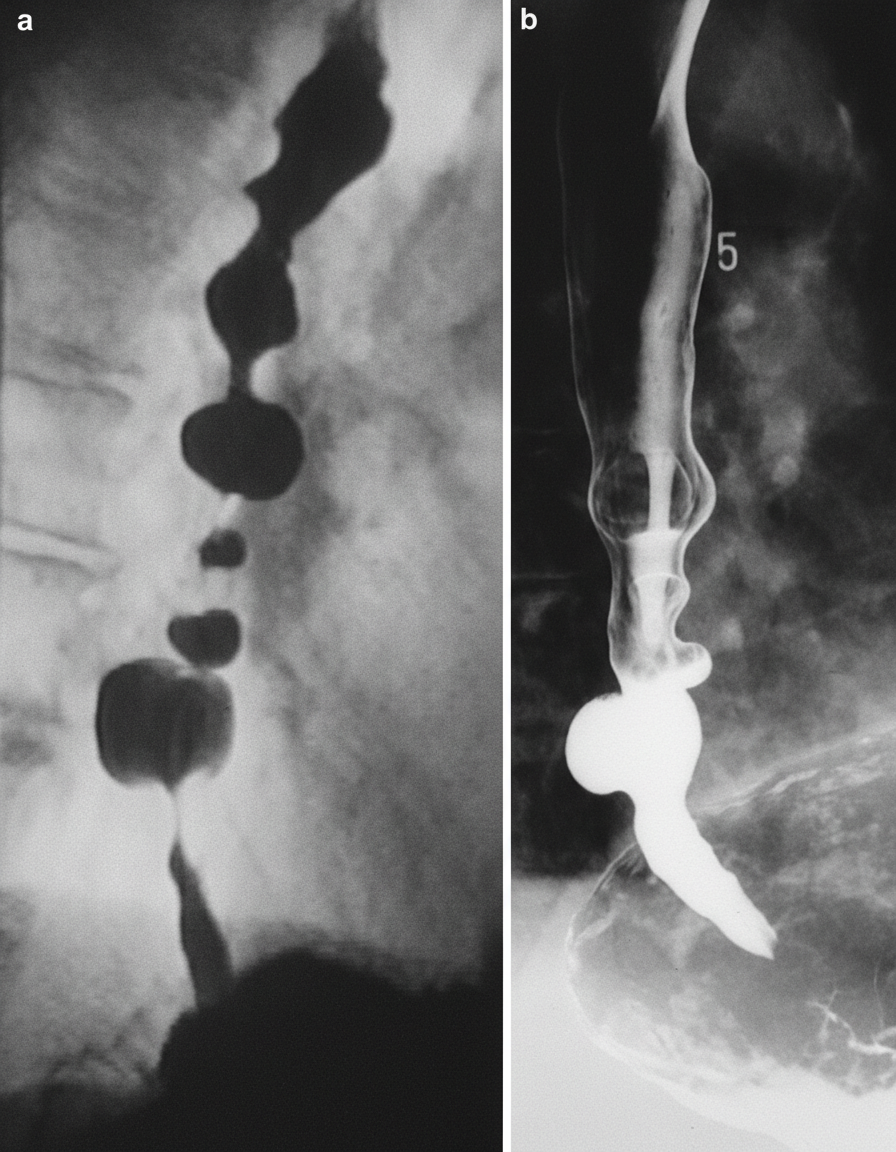
A previously healthy 49-year-old woman comes to the emergency department because of chest pain that radiates to her back. The pain started 45 minutes ago while she was having lunch. Over the past 3 months, she has frequently had the feeling of food, both liquid and solid, getting "stuck" in her chest while she is eating. The patient's vital signs are within normal limits. An ECG shows a normal sinus rhythm with no ST-segment abnormalities. An esophagogram is shown. Further evaluation is most likely to show which of the following?
A 26-year-old male engineer presents to a reproductive specialist due to the inability to conceive after 2 years of trying with his 28-year-old wife. He reports that he is healthy without any significant medical history, surgeries, or medications. He was adopted at 17 years-old. On exam, he is well appearing without dysmorphic features. He has a high pitched voice, absent facial hair, is 5 feet 8 inches tall, and has a BMI of 19 kg/m^2. On genitourinary exam, his testicles are descended bilaterally without varicoceles, and testicular volume is 8cc bilaterally. He has a stretched penile length of 6cm. He has labwork from his primary care physician that is significant for low LH, FSH, and testosterone. What is the most likely cause of his infertility?
A recently deceased 92-year-old woman with a history of arrhythmia was discovered to have amyloid deposition in her atria upon autopsy. Upon further examination, there was no amyloid found in any other organs. The peptide at fault was identified and characterized by the pathologist performing the autopsy. Before its eventual deposition in the cardiac atria, which of the following functions was associated with the peptide?
A researcher is studying physiologic and hormonal changes that occur during pregnancy. Specifically, they examine the behavior of progesterone over the course of the menstrual cycle and find that it normally decreases over time; however, during pregnancy this decrease does not occur in the usual time frame. The researcher identifies a circulating factor that appears to be responsible for this difference in progesterone behavior. In order to further examine this factor, the researcher denatures the circulating factor and examines the sizes of its components on a western blot as compared to several other hormones. One of the bands the researcher identifies in this circulating factor is identical to that of another known hormone with which of the following sites of action?
A group of scientists discovered a neurotoxin that prevents neurons from releasing neurotransmitters. They performed a series of experiments to determine the protein that the neurotoxin affected. They used a fluorescent molecule that localizes to synaptic vesicles. In the control experiment, they observed the movement of vesicles from the cell body down the axon and finally to the synapse, and they saw movement from the synapse back to the cell body. When the neurotoxin was applied, the vesicles stopped moving down the axon, but movement back to the cell body still occurred. They also applied tetanospasmin and botulinum toxin to see if these toxins exhibited similar behavior but they did not. Which of the following proteins is most likely affected by this neurotoxin?
Practice by Chapter
Cardiac output determinants
Practice Questions
Starling's law of the heart
Practice Questions
Preload and afterload concepts
Practice Questions
Contractility determinants
Practice Questions
Regulation of blood pressure
Practice Questions
Baroreceptor reflexes
Practice Questions
Neural control of cardiovascular function
Practice Questions
Endothelial function and dysfunction
Practice Questions
Coronary blood flow regulation
Practice Questions
Regional blood flow distribution
Practice Questions
Exercise cardiovascular physiology
Practice Questions
Aging effects on cardiovascular system
Practice Questions
Integrated cardiovascular responses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app