
Cardiovascular — MCQs

On this page
A 72-year-old woman is brought to the emergency department for right hip pain 1 hour after she fell while walking around in her house. She has been unable to stand or walk since the fall. She has hypertension and gout. Her sister died of multiple myeloma at the age of 55 years. Current medications include amlodipine and febuxostat. She does not smoke cigarettes. She drinks a glass of wine daily. Her temperature is 37.3°C (99.1°F), pulse is 101/min, and blood pressure is 128/86 mm Hg. Examination shows right groin tenderness. Range of motion of the right hip is limited by pain. The remainder of the examination shows no abnormalities. A complete blood count and serum creatinine concentration are within the reference range. An x-ray of the hip shows a linear fracture of the right femoral neck. She is scheduled for surgery. Which of the following is the most likely underlying cause of this patient's fracture?
A 16-year-old male comes to his doctor worried that he has not yet gone through puberty. He feels that his genitals are less developed than they should be for his age. On physical exam, you note an absence of facial hair and that his voice has not yet deepened. Your exam confirms that he is Tanner Stage 1. On a thorough review of systems, you learn that the patient has lacked a sense of smell from birth. Which of the following is implicated in the development of this patient's underlying condition?
A 21-year-old man presents to the physician with numbness and weakness in both legs for about a day. He also mentions that both thighs ache. His past medical history is not significant except for some diarrhea about 3 weeks ago. On physical examination, his temperature is 37.2ºC (99.0ºF), pulse rate is 108/min and respiratory rate is 14/min. His blood pressure is 122/82 mm Hg and 100/78 mm Hg in supine and upright positions, respectively. His neurologic evaluation reveals the presence of bilateral symmetrical weakness of the lower limbs, the absence of deep tendon reflexes, and negative Babinski sign. His sensorium and higher brain functions are normal. Which of the following options best explains the pathophysiological mechanism underlying the patient’s clinical features?
In a patient with acute myocardial ischemia, which of the following cardiovascular structures is at greatest risk of damage?
A 66-year-old male presents to the emergency room with shortness of breath with exertion and at rest for the past 5 days. His shortness of breath is mostly at night, and he is also concerned about bilateral leg swelling. He is a heart failure patient who is being managed with oral medication and has been compliant with his drugs. Physical examination reveals an elderly man in respiratory distress with abdominal distention and bilateral pitting ankle edema. Respiratory rate is 32/min, SpO2 is 93% in room air, and coarse crepitations are heard on both lung bases. Pulse rate is 73/min and barely palpable. His blood pressure is 79/54 mm Hg. On auscultation, a blowing holosystolic murmur is heard at the apex radiating to the left axilla. An echocardiography shows an ejection fraction of 18%. The physician decides to include an inotropic agent in his current medication. What would likely result from this intervention?
A 70-year-old woman presents to her primary care physician with sudden episodes of dizziness that resolve in certain positions. On further questioning she describes a false sense of motion with occasional spinning sensation consistent with vertigo. She denies any recent illnesses or hearing loss aside from presbycusis. Her vital signs are normal. During the physical exam the patient reports an episode of vertigo after transitioning from sitting to supine and horizontal nystagmus is concurrently noted. What is the most likely diagnosis?
A 71-year-old man with hypertension comes to the physician for a follow-up examination. Cardiovascular exam shows the point of maximal impulse to be in the mid-axillary line. A transthoracic echocardiogram shows concentric left ventricular hypertrophy with a normal right ventricle. Which of the following is the most likely underlying mechanism of this patient's ventricular hypertrophy?
A 49-year-old woman presents to the office because of tremors for 2 months. She says that her hands have been shaking a lot, especially when she feels stressed. In addition, she has been sweating more than usual and has lost 8 kg (17.6 lb) in the last 2 months. She has a past medical history of vitiligo. Her vital signs are a heart rate of 98/min, a respiratory rate of 14/min, a temperature of 37.6°C (99.7°F), and a blood pressure of 115/75 mm Hg. Physical examination shows a fine, bilateral hand tremor and a diffuse goiter. Which of the following hormonal imbalances is most likely present?
A previously healthy 57-year-old man comes to the emergency department because of acute retrosternal chest pain that radiates to his back. The pain started suddenly while he was having dinner. A few moments prior to the onset of the pain, he experienced discomfort when trying to eat or drink anything. On the way to the hospital he took a sublingual nitrate tablet that he had at home, which helped relieve the pain. His pulse is 80/min, respirations are 14/min, and blood pressure is 144/88 mm Hg. Examination shows no other abnormalities. An ECG shows a normal sinus rhythm with no ST-segment abnormalities. An esophagogram is done and shows areas of diffuse, uncoordinated spasms in several segments along the length of the esophagus. This patient's condition is most likely to show which of the following findings?
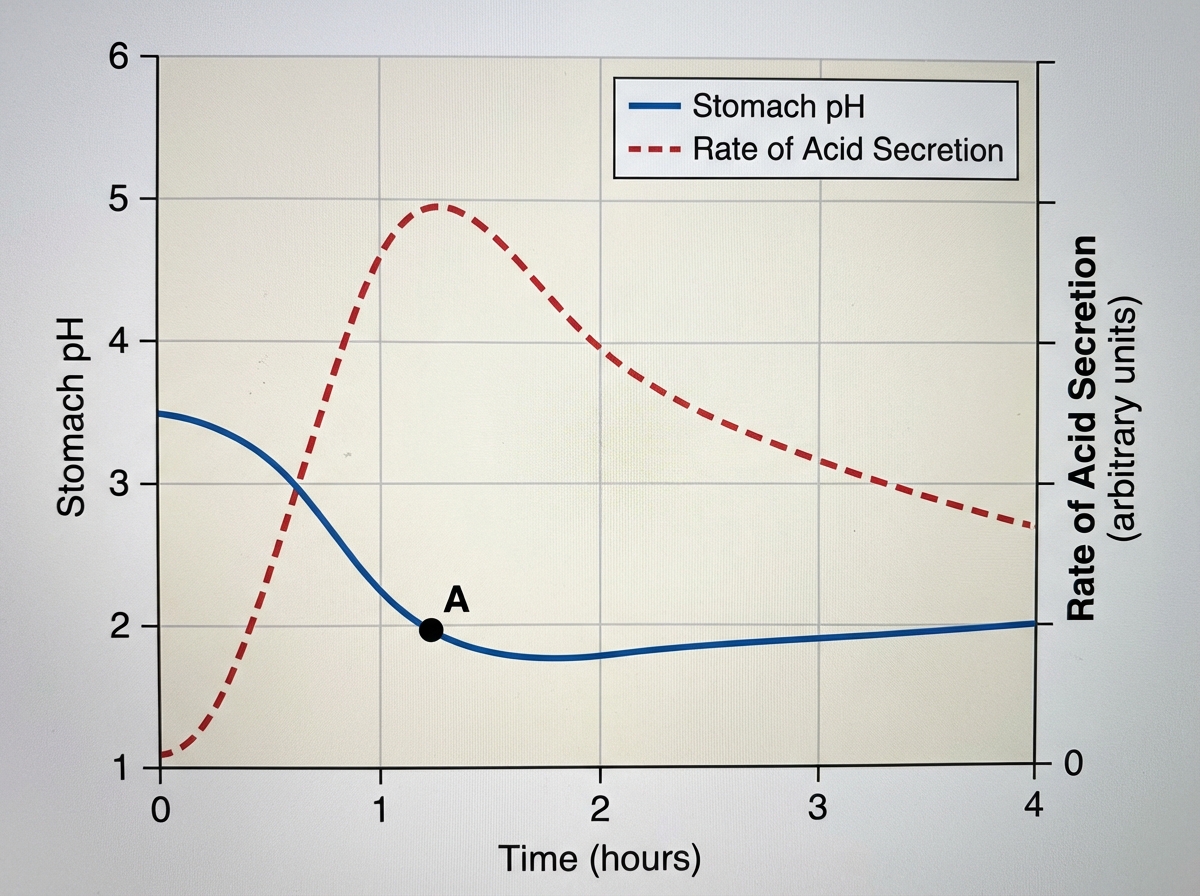
Nine healthy subjects participate in a study of gastric secretions. Subjects are asked to eat a meal at hour 0, at which time the pH of stomach contents and rate of stomach acid secretions are measured over the next 4 hours. Results of the study are shown. Which of the following mediators most directly stimulates the high rate of gastric acid secretion at point A in the graph?
Practice by Chapter
Cardiac output determinants
Practice Questions
Starling's law of the heart
Practice Questions
Preload and afterload concepts
Practice Questions
Contractility determinants
Practice Questions
Regulation of blood pressure
Practice Questions
Baroreceptor reflexes
Practice Questions
Neural control of cardiovascular function
Practice Questions
Endothelial function and dysfunction
Practice Questions
Coronary blood flow regulation
Practice Questions
Regional blood flow distribution
Practice Questions
Exercise cardiovascular physiology
Practice Questions
Aging effects on cardiovascular system
Practice Questions
Integrated cardiovascular responses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app