
Cardiovascular — MCQs

On this page
A 2-month-old girl with a previous diagnosis of DiGeorge syndrome is brought to the emergency department with her parents following a seizure. Her mother states that the baby had been inconsolable all day and refused to feed. She was born at 39 weeks gestation via spontaneous vaginal delivery. She is up to date on all vaccines. Upon arrival to the hospital her heart rate is 120/min, respiratory rate is 40/min, and temperature of 37.0°C (98.6°F). On examination, she is afebrile and somnolent and her fontanelles are open and soft. While attempting to take her blood pressure, the patient’s arm and hand flex sharply and do not relax until the cuff is released. A light tap on the cheek results in an atypical facial muscle twitch. A CMP and CBC are drawn and sent for analysis. Which of the following is the most likely cause?
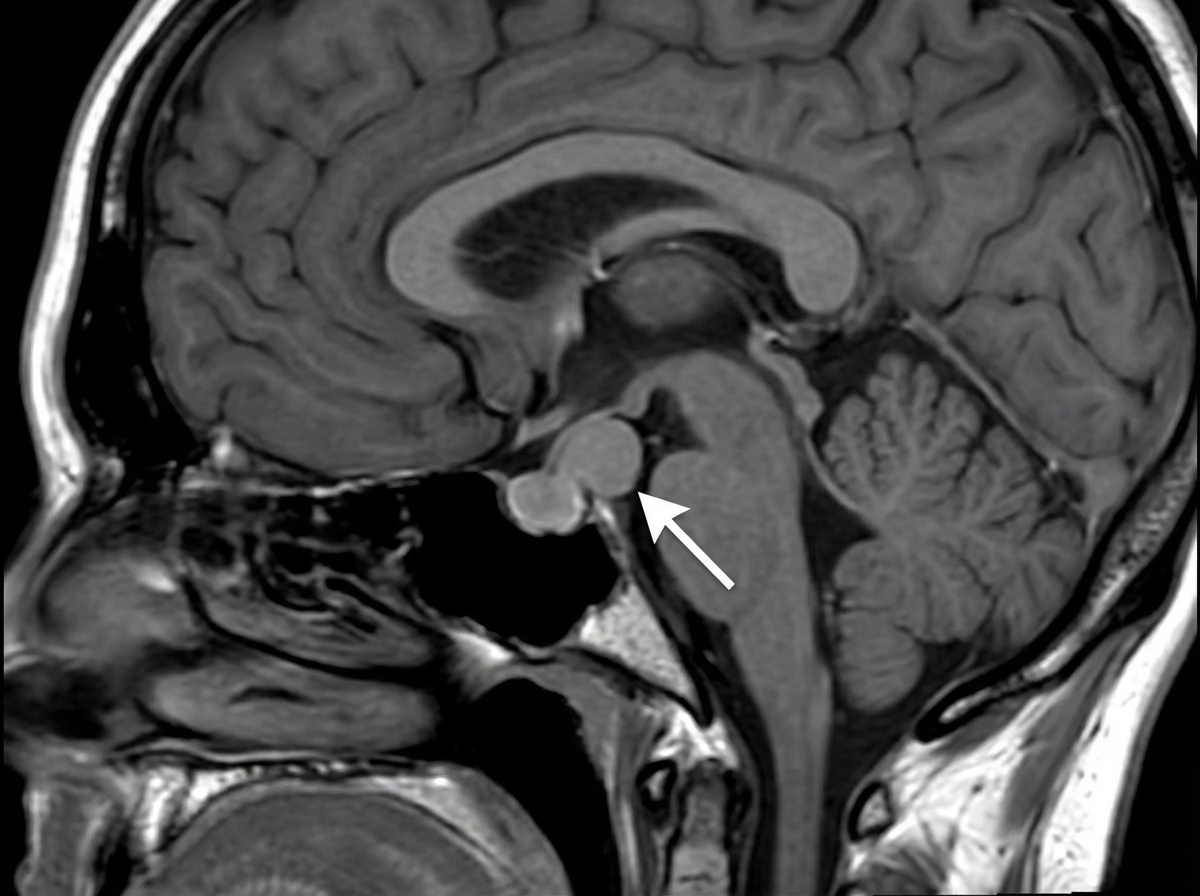
A 17-year-old teenager presents to the clinic with her parents complaining of headaches and loss of vision which began insidiously 3 months ago. She describes her headaches as throbbing, mostly on her forehead, and severe enough to affect her daily activities. She has not experienced menarche. Past medical history is noncontributory. She takes no medication. Both of her parents are alive and well. Today, her blood pressure is 110/70 mm Hg, the heart rate is 90/min, the respiratory rate is 17/min, and the temperature is 37.0°C (98.6°F). Breasts development is in Tanner stage I. Blood work is collected and an MRI is performed (the result is shown). Decreased production of which of the following hormones most likely explains the patient's absent breast development and primary amenorrhea?
A 22-year-old man comes to the physician because of a 2-month history of episodes of shortness of breath, lightheadedness, and palpitations. During the examination, he reports the onset of one such episode. His pulse is 170/min and regular, respirations are 22/min, and blood pressure is 100/65 mm Hg. An ECG shows a regular narrow complex tachycardia; no P waves are visible. A common clinical maneuver to diagnose and/or relieve the patient's symptoms involves stimulation of which of the following nerves?
Under what physiologic state is the endogenous human analog of nesiritide produced?
A 42-year-old woman presents to her primary care physician with 2 weeks of abdominal pain. She says that the pain is squeezing in character and gets worse after she eats food. The pain is particularly bad after she eats dairy products so she has begun to avoid ice cream and cheese. Furthermore, she has noticed that she has been experiencing episodes of nausea associated with abdominal pain in the last 4 days. Physical exam reveals tenderness to palpation and rebound tenderness in the right upper quadrant of the abdomen. The molecule that is most likely responsible for the increased pain this patient experiences after eating fatty foods is most likely secreted by which of the following cells?
Paramedics respond to a call regarding an 18-year-old male with severe sudden-onset heart palpitations. The patient reports symptoms of chest pain, fatigue, and dizziness. Upon examination, his heart rate is 175/min and regular. His blood pressure is 110/75 mm Hg. Gentle massage below the level of the left mandible elicits an immediate improvement in the patient, as his heart rate returns to 70/min. What was the mechanism of action of this maneuver?
A 72-year-old man comes to the physician for a routine physical examination. He does not take any medications. Physical examination shows no abnormalities. Laboratory studies show a calcium concentration of 8.5 mg/dL, a phosphorus concentration of 3.1 mg/dL, an elevated bone-specific alkaline phosphatase concentration, and a normal urine deoxypyridinoline concentration. Which of the following is the most likely explanation for this patient's laboratory abnormalities?
A 45-year-old executive travels frequently around the world. He often has difficulty falling asleep at night when he returns home. You suspect a circadian rhythm disorder is responsible for his pathology. Which of the following regulates the circadian rhythm?
A 47-year-old Hispanic man presents with complaints of recent heat intolerance and rapid heart rate. The patient has also experienced recent unintentional weight loss of 15 pounds. Physical exam reveals tachycardia and skin that is warm to the touch. A radioactive iodine uptake scan of the thyroid reveals several focal nodules of increased iodine uptake. Prior to this study, the physician had also ordered a serum analysis that will most likely show which of the following?
A 70 year-old man comes to the physician for difficulty swallowing for 6 months. During this time, he has occasionally coughed up undigested food. He did not have weight loss or fever. Four weeks ago, he had an episode of sore throat, that resolved spontaneously. He has smoked one pack of cigarettes daily for 5 years. He has gastroesophageal reflux disease and osteoporosis. Current medications include alendronate and omeprazole. His temperature is 37.0°C (98.6°F), pulse is 84/min, and blood pressure is 130/90 mmHg. On examination, he has foul-smelling breath and a fluctuant mass on the right neck. Which of the following is most likely involved in the pathogenesis of this patient's symptoms?
Practice by Chapter
Cardiac output determinants
Practice Questions
Starling's law of the heart
Practice Questions
Preload and afterload concepts
Practice Questions
Contractility determinants
Practice Questions
Regulation of blood pressure
Practice Questions
Baroreceptor reflexes
Practice Questions
Neural control of cardiovascular function
Practice Questions
Endothelial function and dysfunction
Practice Questions
Coronary blood flow regulation
Practice Questions
Regional blood flow distribution
Practice Questions
Exercise cardiovascular physiology
Practice Questions
Aging effects on cardiovascular system
Practice Questions
Integrated cardiovascular responses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app