
Cardiovascular — MCQs

On this page
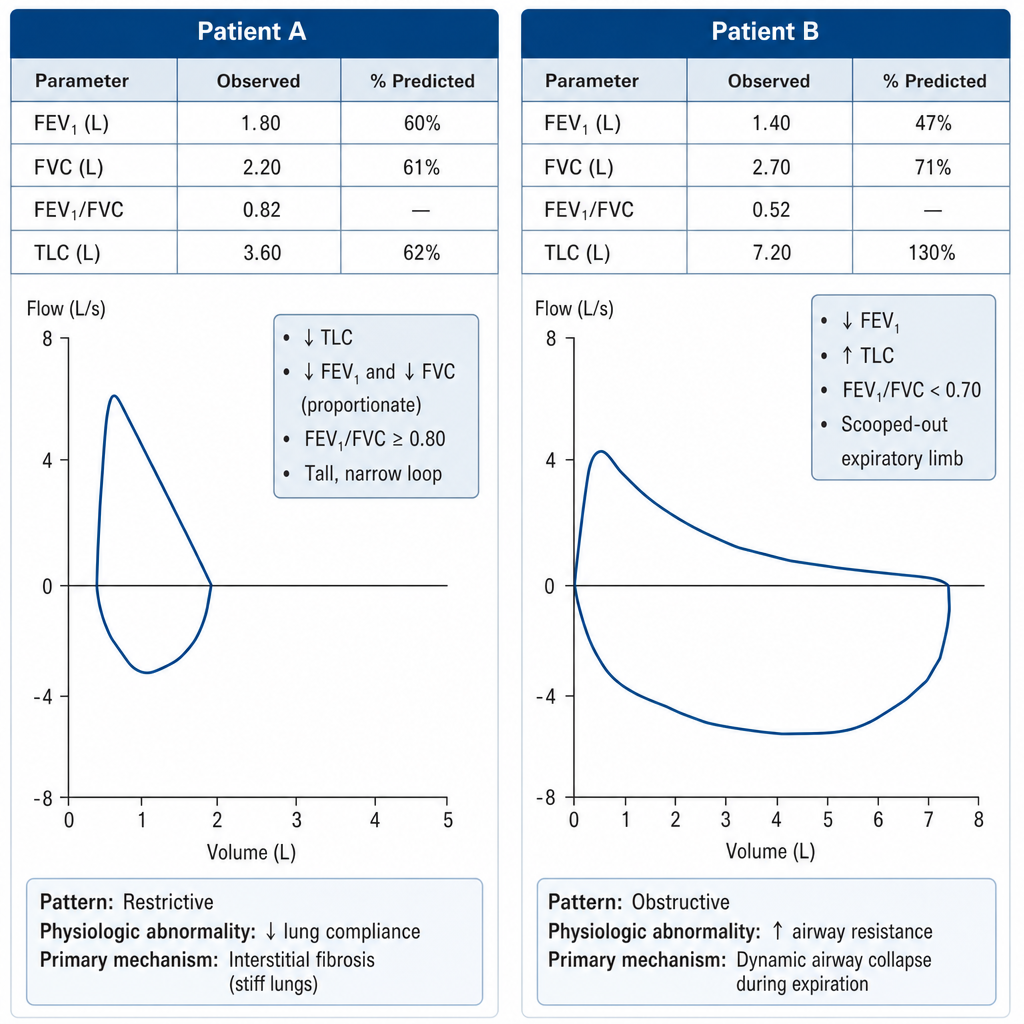
A pulmonologist reviews spirometry tracings from two patients with dyspnea. Patient A's loop shows a reduced total lung capacity, proportionally reduced FEV1 and FVC with an FEV1/FVC ratio of 0.82, and a tall, narrow loop shape. Patient B's loop shows a reduced FEV1, increased TLC, a scooped-out expiratory limb, and an FEV1/FVC ratio of 0.52. Which of the following correctly pairs each patient with the underlying physiological abnormality and its primary mechanism?
A 33-year-old woman presents to her physician's office for a postpartum check-up. She gave birth to a full-term boy via an uncomplicated vaginal delivery 3 weeks ago and has been exclusively breastfeeding her son. The hormone most responsible for promoting milk let-down during lactation in this new mother would lead to the greatest change in the level of which of the following factors?
A 68-year-old man is brought to the emergency department 30 minutes after collapsing on the street. On arrival, he is obtunded. His pulse is 110/min and blood pressure is 250/120 mm Hg. A CT scan of the head shows an intracerebral hemorrhage involving bilateral thalamic nuclei and the third ventricle. Cortical detection of which of the following types of stimuli is most likely to remain unaffected in this patient?
A medical student volunteers for an experiment in the physiology laboratory. Before starting the experiment, her oral temperature is recorded as 36.9°C (98.4°F). She is then made to dip both her hands in a bowl containing ice cold water. She withdraws her hands out of the water, and finds that they look pale and feel very cold. Her oral temperature is recorded once more and is found to be 36.9°C (98.4°F) even though her hands are found to be 4.5°C (40.0°F). Which of the following mechanisms is responsible for the maintenance of her temperature throughout the experiment?
A previously healthy 35-year-old woman comes to the physician because of palpitations and anxiety for the past 2 months. She has had a 3.1-kg (7-lb) weight loss in this period. Her pulse is 112/min. Cardiac examination shows normal heart sounds with a regular rhythm. Neurologic examination shows a fine resting tremor of the hands; patellar reflexes are 3+ bilaterally with a shortened relaxation phase. Urine pregnancy test is negative. Which of the following sets of laboratory values is most likely on evaluation of blood obtained before treatment? | TSH | Free T4 | Free T3 | Thyroxine-binding globulin |
A 50-year-old man presents to the emergency department due to altered mental status. His symptoms began approximately two weeks prior to presentation where he complained of increasing fatigue, malaise, loss of appetite, and subjective fever. Vital signs are significant for a temperature of 102.0°F (38.9°C). On physical examination, there is a holosystolic murmur in the tricuspid area, linear non-blanching reddish lesions under the nails, and needle tracks on both antecubital fossa. A transthoracic echocardiogram shows a vegetation on the tricuspid valve. Blood cultures return positive for Staphylococcus aureus. A lumbar puncture is prompted due to altered mental status in the setting of fever; however, there is no bacteria found on cerebral spinal fluid (CSF) culture. Which of the following cell structures prevents the penetration of the bacteria into the CSF from his blood?
A 32-year-old woman presents to the clinic with complaints of insomnia, diarrhea, anxiety, thinning hair, and diffuse muscle weakness. She has a family history of type 1 diabetes mellitus and thyroid cancer. She drinks 1–2 glasses of wine weekly. Her vital signs are unremarkable. On examination, you notice that she also has bilateral exophthalmos. Which of the following results would you expect to see on a thyroid panel?
A 60-year-old obese man comes to the emergency department with tightness in his chest and lower extremity edema. He has a history of heart failure that has gotten worse over the last several years. He takes finasteride, lisinopril, and albuterol. He does not use oxygen at home. He has mildly elevated blood pressure, and he is tachycardic and tachypneic. Physical examination shows an overweight man having difficulty speaking with 2+ pitting edema on his lower extremities up to his thighs. The attending asks you to chart out the patient's theoretical cardiac function curve from where it was 5 years ago when he was healthy to where it is right now. What changes occurred in the last several years without compensation?
You have been asked to deliver a lecture to medical students about the effects of various body hormones and neurotransmitters on the metabolism of glucose. Which of the following statements best describes the effects of sympathetic stimulation on glucose metabolism?
A 12-year-old girl is brought to the emergency department 3 hours after the sudden onset of colicky abdominal pain and vomiting. She also has redness and swelling of the face and lips without pruritus. Her symptoms began following a tooth extraction earlier this morning. She had a similar episode of facial swelling after a bicycle accident 1 year ago which resolved within 48 hours without treatment. Vital signs are within normal limits. Examination shows a nontender facial edema, erythema of the oral mucosa, and an enlarged tongue. The abdomen is soft and there is tenderness to palpation over the lower quadrants. An abdominal ultrasound shows segmental thickening of the intestinal wall. Which of the following is the most likely cause of this patient's condition?
Practice by Chapter
Cardiac output determinants
Practice Questions
Starling's law of the heart
Practice Questions
Preload and afterload concepts
Practice Questions
Contractility determinants
Practice Questions
Regulation of blood pressure
Practice Questions
Baroreceptor reflexes
Practice Questions
Neural control of cardiovascular function
Practice Questions
Endothelial function and dysfunction
Practice Questions
Coronary blood flow regulation
Practice Questions
Regional blood flow distribution
Practice Questions
Exercise cardiovascular physiology
Practice Questions
Aging effects on cardiovascular system
Practice Questions
Integrated cardiovascular responses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app