
Systolic function assessment — MCQs

A previously healthy 19-year-old man is brought to the emergency department by his girlfriend after briefly losing consciousness. He passed out while moving furniture into her apartment. She said that he was unresponsive for a minute but regained consciousness and was not confused. The patient did not have any chest pain, palpitations, or difficulty breathing before or after the episode. He has had episodes of dizziness when exercising at the gym. His blood pressure is 125/75 mm Hg while supine and 120/70 mm Hg while standing. Pulse is 70/min while supine and 75/min while standing. On examination, there is a grade 3/6 systolic murmur at the left lower sternal border and a systolic murmur at the apex, both of which disappear with passive leg elevation. Which of the following is the most likely cause?
A 49-year-old man presents to his physician complaining of weakness and fatigue. On exam, you note significant peripheral edema. Transthoracic echocardiogram is performed and reveals a preserved ejection fraction with impaired diastolic relaxation. A representative still image is shown in Image A. Which of the following is likely the cause of this patient's symptoms?
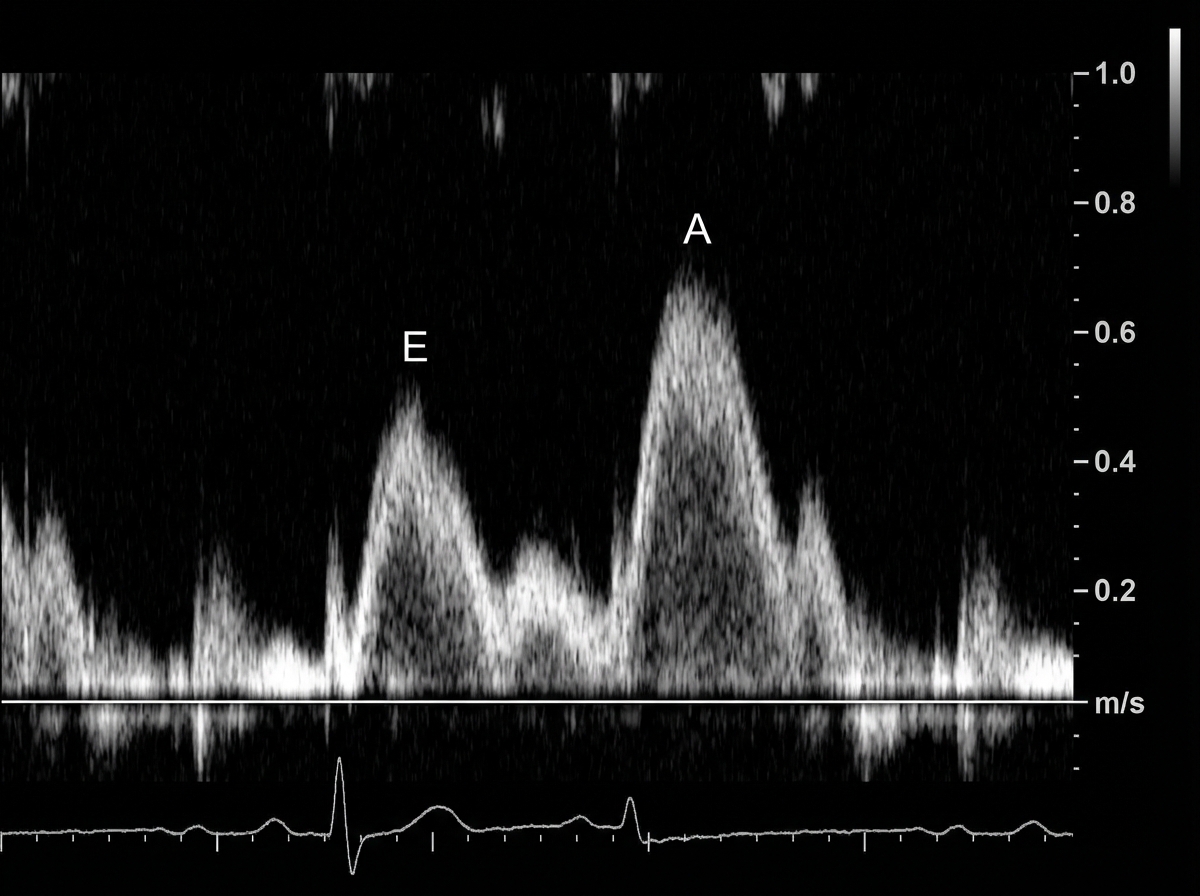
The serum brain natriuretic peptide and N-terminal pro-BNP are elevated. A diagnosis of heart failure with preserved ejection fraction is made. In addition to supplemental oxygen therapy, which of the following is the most appropriate initial step in management?
A 60-year-old male engineer who complains of shortness of breath when walking a few blocks undergoes a cardiac stress test because of concern for coronary artery disease. During the test he asks his cardiologist about what variables are usually used to quantify the functioning of the heart. He learns that one of these variables is stroke volume. Which of the following scenarios would be most likely to lead to a decrease in stroke volume?
A 73-year-old woman presents to clinic with a week of fatigue, headache, and swelling of her ankles bilaterally. She reports that she can no longer go on her daily walk around her neighborhood without stopping frequently to catch her breath. At night she gets short of breath and has found that she can only sleep well in her recliner. Her past medical history is significant for hypertension and a myocardial infarction three years ago for which she had a stent placed. She is currently on hydrochlorothiazide, aspirin, and clopidogrel. She smoked 1 pack per day for 30 years before quitting 10 years ago and socially drinks around 1 drink per month. She denies any illicit drug use. Her temperature is 99.0°F (37.2°C), pulse is 115/min, respirations are 18/min, and blood pressure is 108/78 mmHg. On physical exam there is marked elevations of her neck veins, bilateral pitting edema in the lower extremities, and a 3/6 holosystolic ejection murmur over the right sternal border. Echocardiography shows the following findings: End systolic volume (ESV): 100 mL End diastolic volume (EDV): 160 mL How would cardiac output be determined in this patient?
In a patient with acute myocardial ischemia, which of the following cardiovascular structures is at greatest risk of damage?
A researcher is studying how electrical activity propagates across the heart. In order to do this, he decides to measure the rate at which an action potential moves within various groups of cardiac muscle tissue. In particular, he isolates fibers from areas of the heart with the following characteristics: A) Dysfunction leads to fixed PR intervals prior to a dropped beat B) Dysfunction leads to increasing PR intervals prior to a dropped beat C) Dysfunction leads to tachycardia with a dramatically widened QRS complex D) Dysfunction leads to tachycardia with a sawtooth pattern on electrocardiogram Which of the following is the proper order of these tissues from fastest action potential propagation to slowest action potential propagation.
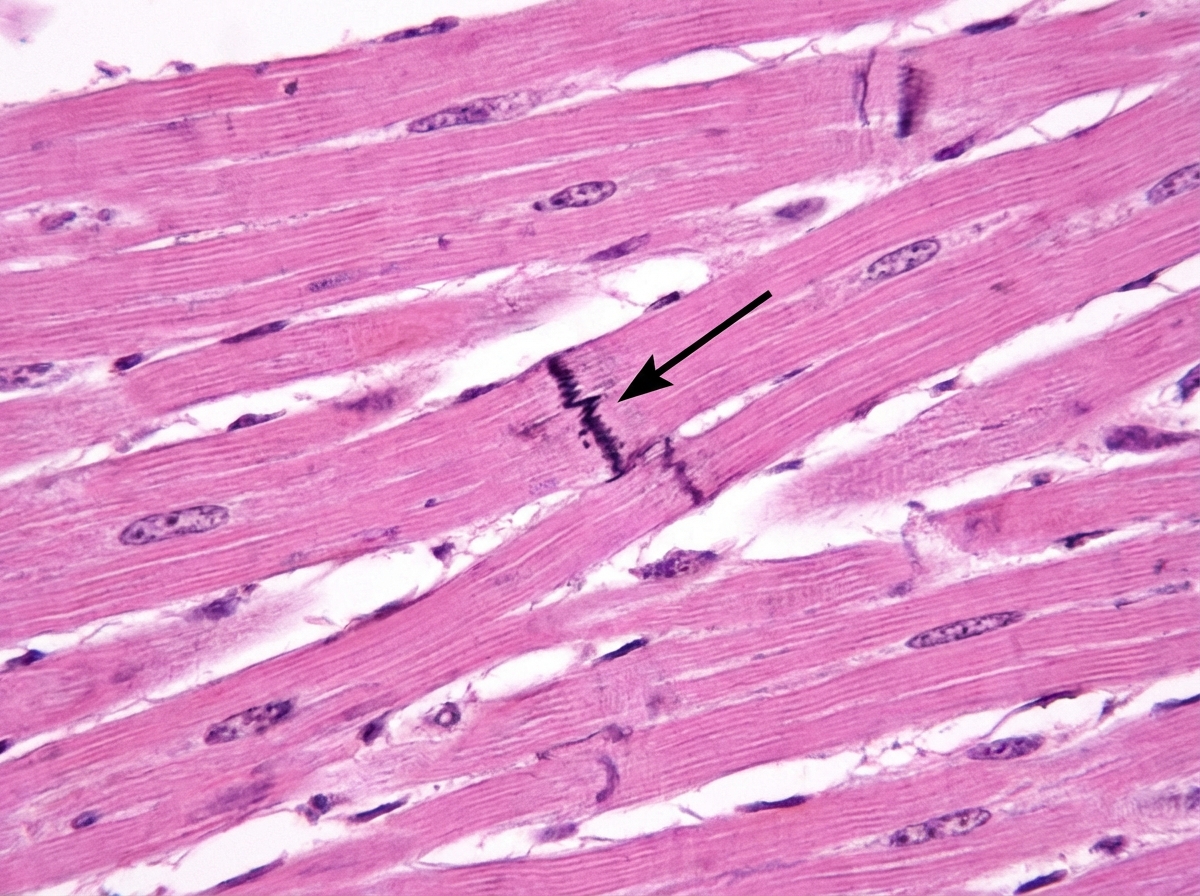
Cardiac muscle serves many necessary functions, leading to a specific structure that serves these functions. The structure highlighted is an important histology component of cardiac muscle. What would be the outcome if this structure diffusely failed to function?
A 36-year-old woman is admitted to the hospital for the evaluation of progressive breathlessness. She has no history of major medical illness. Her temperature is 37°C (98.6°F), pulse is 110/min, and respirations are 22/min. Pulse oximetry on room air shows an oxygen saturation of 99%. Cardiac examination shows a loud S1 and S2. There is a grade 2/6 early systolic murmur best heard in the 2nd right intercostal space. Cardiac catheterization shows a mixed venous oxygen saturation of 55% (N= 65–70%). Which of the following is the most likely cause of this patient's breathlessness?
A 72-year-old man with severe aortic regurgitation and compensated heart failure is being evaluated for surgical intervention. His echocardiogram shows LV end-diastolic dimension of 7.5 cm, ejection fraction of 45%, and severe aortic regurgitation with a regurgitant fraction of 60%. Pressure-volume loop analysis shows a markedly widened loop with increased stroke work. Evaluate the compensatory mechanisms maintaining his cardiac output and predict the timing for surgical intervention based on cardiac cycle mechanics.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app