
Cardiac cycle — MCQs

On this page
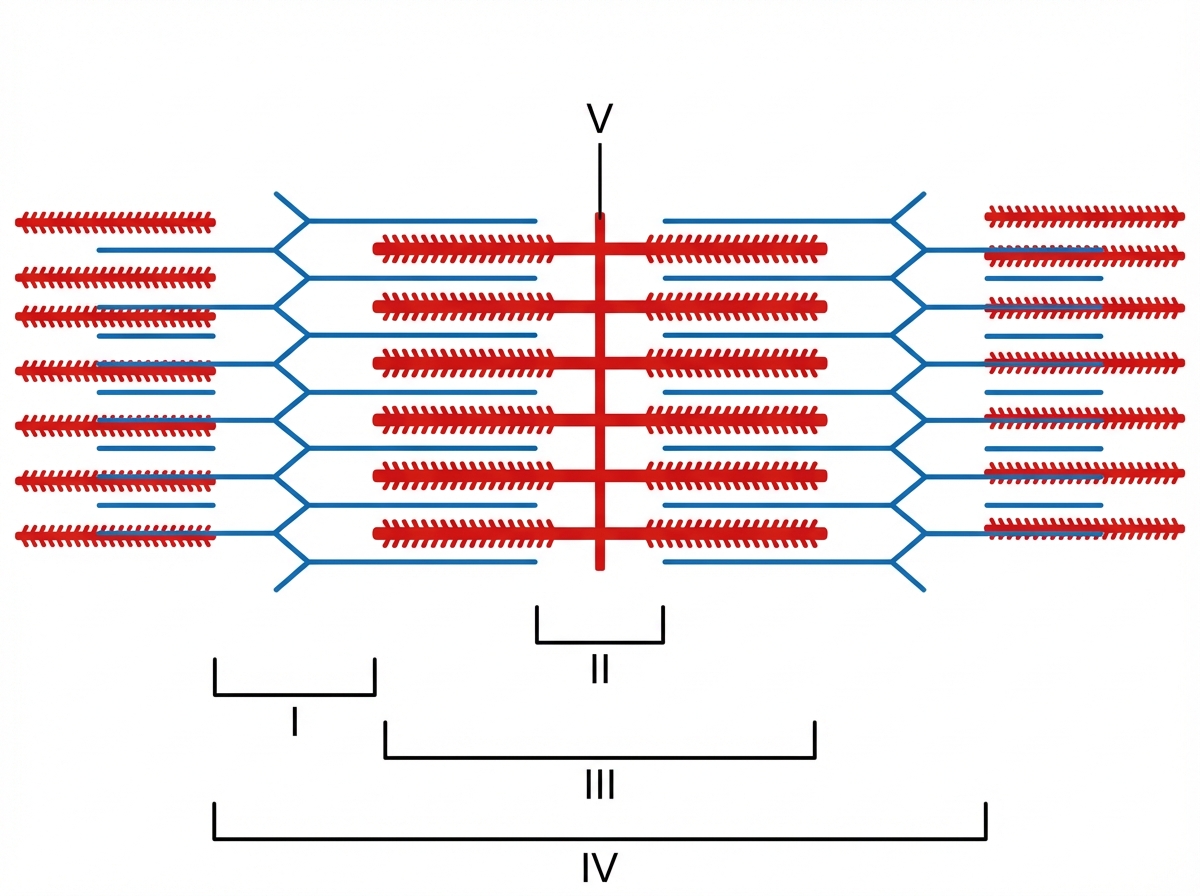
An energy drink claiming to improve athletic performance is being investigated for its mechanism of action. An active substance in the drink is thought to increase the activity of an ATPase involved in muscle contraction. Radiolabeling of the active substance reveals it binds to an allosteric site on the globular head of a myosin heavy chain dimer, with greater affinity during muscle relaxation and lesser affinity when the myosin head binds actin. During muscle relaxation, what portion of the sarcomere shown below will exhibit the greatest affinity for the substance?
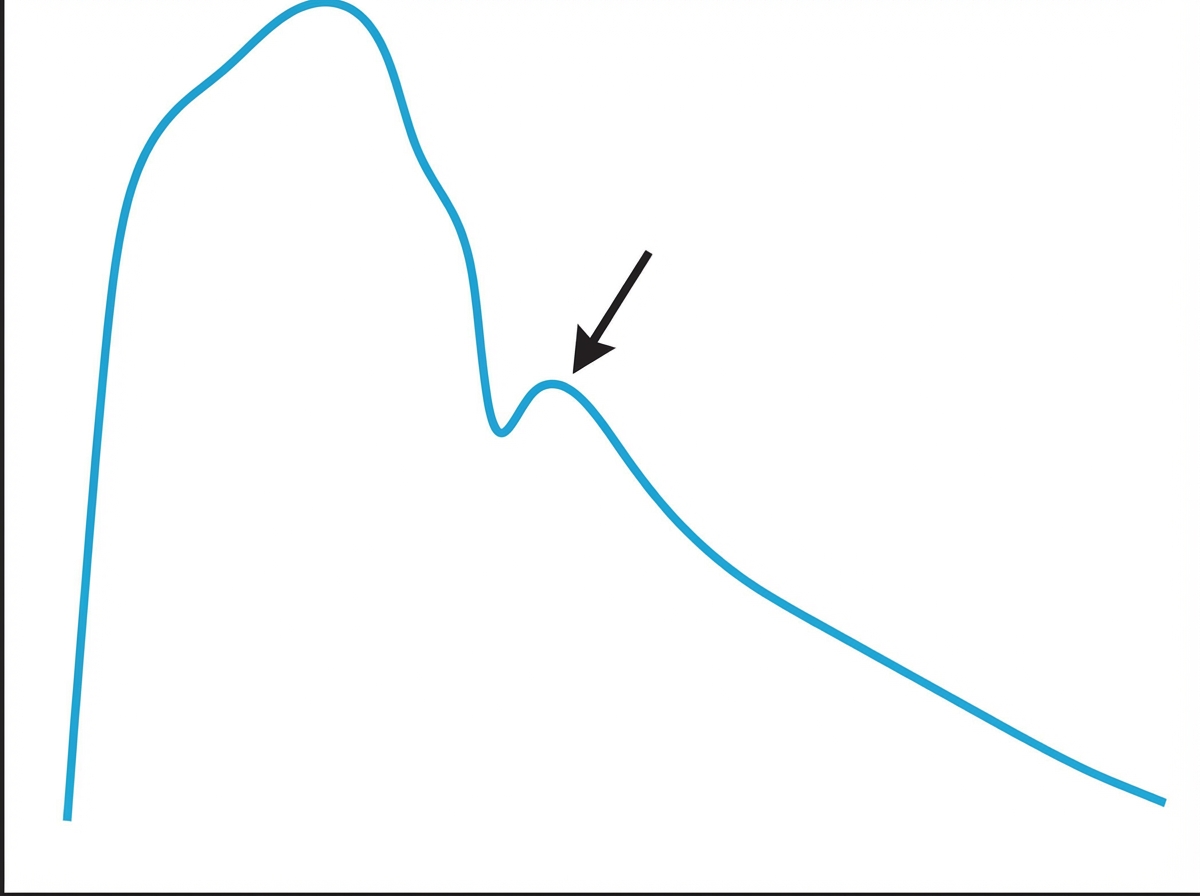
Prior to undergoing a total knee arthroplasty, a 62-year-old man with coronary artery disease undergoes diagnostic cardiac catheterization. The catheter is inserted via the femoral artery and then advanced to the ascending aorta. Pressure tracing of the catheter is shown. The peak marked by the arrow is most likely caused by which of the following?
A 21-year-old man presents to his physician for a routine checkup. His doctor asks him if he has had any particular concerns since his last visit and if he has taken any new medications. He says that he has not been ill over the past year, except for one episode of the flu. He has been training excessively for his intercollege football tournament, which is supposed to be a huge event. His blood pressure is 110/70 mm Hg, pulse is 69/min, and respirations are 17/min. He has a heart sound coinciding with the rapid filling of the ventricles and no murmurs. He does not have any other significant physical findings. Which of the following best describes the heart sound heard in this patient?
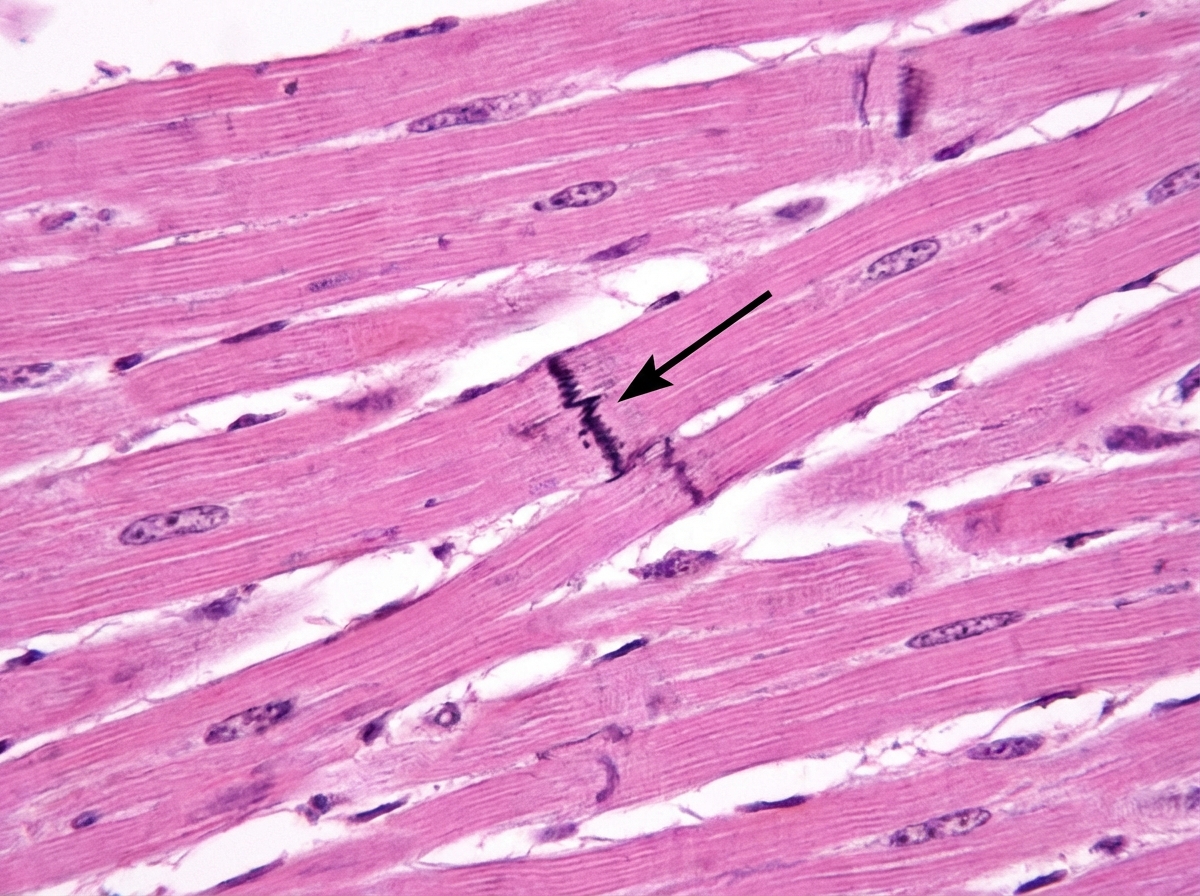
Cardiac muscle serves many necessary functions, leading to a specific structure that serves these functions. The structure highlighted is an important histology component of cardiac muscle, specifically its gap junctions. What would be the outcome if this structure diffusely failed to function?
A molecular biologist is studying the roles of different types of ion channels regulating cardiac excitation. He identifies a voltage-gated calcium channel in the sinoatrial node, which is also present throughout the myocardium. The channel is activated at ~ -40 mV of membrane potential, undergoes voltage-dependent inactivation, and is highly sensitive to nifedipine. Which of the following phases of the action potential in the sinoatrial node is primarily mediated by ion currents through the channel that the molecular biologist is studying?
A 21-year-old man presents to a physician with repeated episodes of syncope and dizziness over the last month. On physical examination, his pulse is 64/min while all other vital signs are normal. His 24-hour ECG monitoring suggests a diagnosis of sinus node dysfunction. His detailed genetic evaluation shows that he carries a copy of a mutated gene “X” that codes for an ion channel, which is the most important ion channel underlying the automaticity of the sinoatrial node. This is the first ion channel to be activated immediately after hyperpolarization. Which of the following ion channels does the gene “X” code for?
A 27-year-old man presents to the clinic for his annual physical examination. He was diagnosed with a rare arrhythmia a couple of years ago following an episode of dizziness. A mutation in the gene encoding for the L-type calcium channel protein was identified by genetic testing. He feels fine today. His vitals include: blood pressure 122/89 mm Hg, pulse 90/min, respiratory rate 14/min, and temperature 36.7°C (98.0°F). The cardiac examination is unremarkable. The patient has been conducting some internet research on how the heart works and specifically asks you about his own “ventricular action potential”. Which of the following would you expect to see in this patient?
While explaining the effects of hypokalemia and hyperkalemia on the cardiac rhythm, a cardiologist explains that the electrophysiology of cardiac tissue is unique. He mentions that potassium ions play an important role in the electrophysiology of the heart, and the resting membrane potential of the cardiac myocytes is close to the equilibrium potential of K+ ions. This is because of the high resting potassium conductance of the ventricular myocytes, which is regulated by specific potassium channels. These are open at rest and are closed when there is depolarization. Which of the following potassium channels is the cardiologist talking about?
A woman with coronary artery disease is starting to go for a walk. As she begins, her heart rate accelerates from a resting pulse of 60 bpm until it reaches a rate of 120 bpm, at which point she begins to feel a tightening in her chest. She stops walking to rest and the tightening resolves. This has been happening to her consistently for the last 6 months. Which of the following is a true statement?
Practice by Chapter
Phases of the cardiac cycle
Practice Questions
Pressure-volume relationships
Practice Questions
Heart sounds and their origin
Practice Questions
Ventricular filling dynamics
Practice Questions
Valve function during cardiac cycle
Practice Questions
Electrical-mechanical coupling
Practice Questions
Isovolumetric contraction and relaxation
Practice Questions
Ventricular ejection physiology
Practice Questions
Atrial contribution to cardiac function
Practice Questions
Cardiac cycle in pathologic states
Practice Questions
Diastolic function assessment
Practice Questions
Systolic function assessment
Practice Questions
Effects of heart rate on cardiac cycle
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app