
Heart sounds and their origin — MCQs

A 73-year-old man presents to your clinic for a routine checkup. His medical history is notable for a previous myocardial infarction. He states that he has not seen a doctor in "many years". He has no complaints. When you auscultate over the cardiac apex with the bell of your stethoscope, you notice an additional sound immediately preceding S1. This extra heart sound is most likely indicative of which of the following processes?
A 64-year-old man presents to the emergency department because he has been experiencing increased shortness of breath for the last 2 weeks. Specifically, he says that he can barely walk up the stairs to his apartment before he feels winded. In addition, he has been waking up at night gasping for breath and has only been able to sleep propped up on 2 more pillows than usual. Physical exam reveals jugular venous distention as well as pitting lower extremity edema. Which of the following abnormal sounds will most likely be heard in this patient?
A 31-year-old woman presents to the clinic with shortness of breath, palpitations, and fatigue. She has had these symptoms over the last several weeks. She had been tolerating these symptoms until last night when she could not fall asleep due to palpitations. She has a past medical history of infective endocarditis 6 months ago that was successfully treated with antibiotics. She does not smoke or drink alcohol. Her blood pressure is 138/89 mm Hg and her pulse is 76/min and regular. The cardiac exam reveals a soft S1, S3 gallop, a hyperdynamic apex beat, and a pansystolic murmur that radiates to the axilla on auscultation. Echocardiography reveals incompetence of one of the valves. Which of the following sites is the best position to auscultate this defect?
A 21-year-old man presents to his physician for a routine checkup. His doctor asks him if he has had any particular concerns since his last visit and if he has taken any new medications. He says that he has not been ill over the past year, except for one episode of the flu. He has been training excessively for his intercollege football tournament, which is supposed to be a huge event. His blood pressure is 110/70 mm Hg, pulse is 69/min, and respirations are 17/min. He has a heart sound coinciding with the rapid filling of the ventricles and no murmurs. He does not have any other significant physical findings. Which of the following best describes the heart sound heard in this patient?
A 74-year-old man comes to the physician for a 6-month history of progressively worsening fatigue and shortness of breath on exertion. He immigrated to the United States 35 years ago from India. His pulse is 89/min and blood pressure is 145/60 mm Hg. Crackles are heard at the lung bases. Cardiac examination shows a grade 3/6 early diastolic murmur loudest at the third left intercostal space. Further evaluation of this patient is most likely to show which of the following?
A 52-year-old man comes to the physician for a routine health maintenance examination. He has not seen a physician for 10 years. He works as a telemarketer and does not exercise. Cardiac examination shows a dull, low-pitched sound during late diastole that is best heard at the apex. The sound is loudest in the left lateral decubitus position and during end-expiration. Which of the following is the most likely cause of this finding?
A 27-year-old male arrives in the emergency department with a stab wound over the precordial chest wall. The patient is in distress and is cold, sweaty, and pale. Initial physical examination is significant for muffled heart sounds, distended neck veins, and a 3 cm stab wound near the left sternal border. Breath sounds are present bilaterally without evidence of tracheal deviation. Which of the following additional findings would be expected on further evaluation?
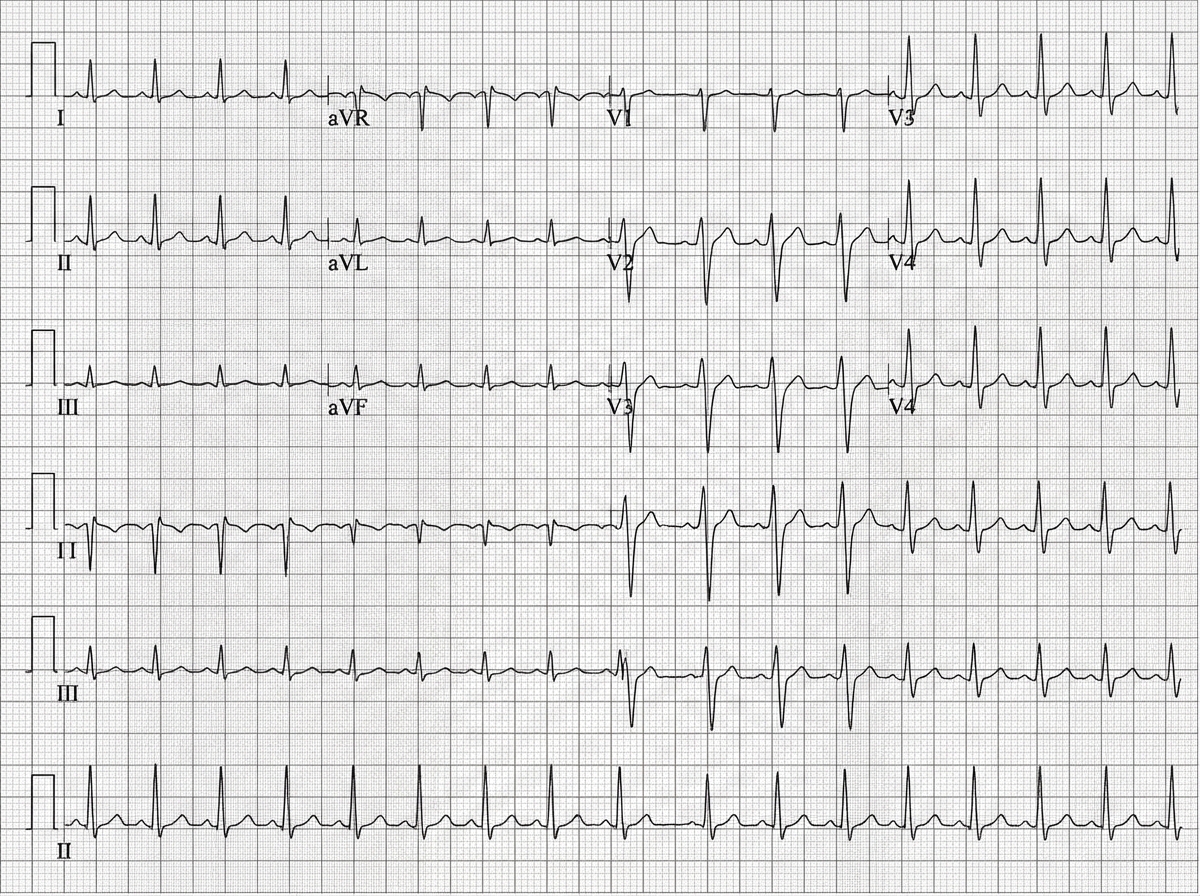
A 45-year-old man is brought to the emergency department after a car accident with pain in the middle of his chest and some shortness of breath. He has sustained injuries to his right arm and leg. He did not lose consciousness. His temperature is 37°C (98.6°F), pulse is 110/min, respirations are 18/min, and blood pressure is 90/60 mm Hg. He is alert and oriented to person, place, and time. Examination shows several injuries to the upper extremities and chest. There are jugular venous pulsations 10 cm above the sternal angle. Heart sounds are faint on cardiac examination. The lungs are clear to auscultation. An ECG is shown. Which of the following is the most appropriate next step in management?
A 65-year-old woman comes to the physician because of a 3-month history of intermittent palpitations and shortness of breath. Cardiopulmonary examination shows no other abnormalities. An ECG shows an absence of P waves, an oscillating baseline, and irregular RR intervals at a rate of approximately 95 beats per minute. The difference between atrial and ventricular rates in this patient is most likely due to which of the following?
A 72-year-old man with severe aortic regurgitation and compensated heart failure is being evaluated for surgical intervention. His echocardiogram shows LV end-diastolic dimension of 7.5 cm, ejection fraction of 45%, and severe aortic regurgitation with a regurgitant fraction of 60%. Pressure-volume loop analysis shows a markedly widened loop with increased stroke work. Evaluate the compensatory mechanisms maintaining his cardiac output and predict the timing for surgical intervention based on cardiac cycle mechanics.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app