
Cardiac cycle in pathologic states — MCQs

A 49-year-old male presents to the emergency room with dyspnea and pulmonary edema. He reports that he has been smoking 2 packs a day for the past 25 years and has difficulty breathing during any sustained physical activity. His blood pressure is normal, and he reports a history of COPD. An echocardiogram was ordered as part of a cardiac workup. Which of the following would be the most likely finding?
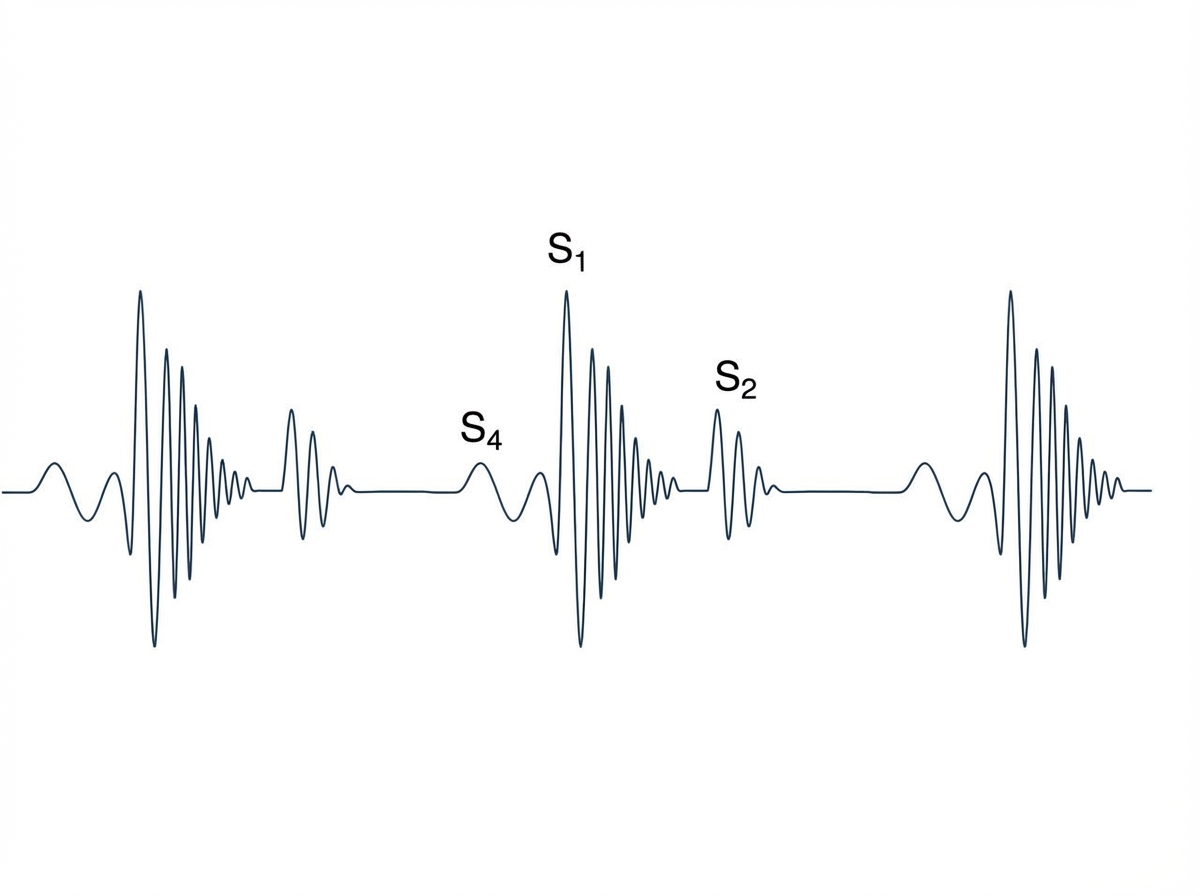
A 67-year-old male with a history of poorly controlled hypertension, COPD, and diabetes presents to his cardiologist for a routine appointment. He reports that he has no current complaints and has not noticed any significant changes in his health. On exam, the cardiologist hears an extra heart sound in late diastole that immediately precedes S1. This heart sound is most associated with which of the following?
A 72-year-old man presents to his primary care physician for a general checkup. The patient works as a farmer and has no concerns about his health. He has a past medical history of hypertension and obesity. His current medications include lisinopril and metoprolol. His temperature is 99.5°F (37.5°C), blood pressure is 177/108 mmHg, pulse is 90/min, respirations are 17/min, and oxygen saturation is 98% on room air. Physical exam is notable for a murmur after S2 over the left sternal border. The patient demonstrates a stable gait and 5/5 strength in his upper and lower extremities. Which of the following is another possible finding in this patient?
A 65-year-old man with hypertension comes to the physician for a routine health maintenance examination. Current medications include atenolol, lisinopril, and atorvastatin. His pulse is 86/min, respirations are 18/min, and blood pressure is 145/95 mm Hg. Cardiac examination is shown. Which of the following is the most likely cause of this physical examination finding?
A 34-year-old male is brought to the emergency department. He has prior hospitalizations for opiate overdoses, but today presents with fever, chills, rigors and malaise. On physical exam vitals are temperature: 100.5 deg F (38.1 deg C), pulse is 105/min, blood pressure is 135/60 mmHg, and respirations are 22/min. You note the following findings on the patient's hands (Figures A and B). You note that as the patient is seated, his head bobs with each successive heart beat. Which of the following findings is most likely present in this patient?

A 54-year-old woman presents to the emergency ward with a chief complaint of chest pain. The pain is sharp and present in the anterior part of the chest. There is no radiation of the pain; however, the intensity is decreased while sitting and leaning forward. There is no associated shortness of breath. Vital signs are the following: blood pressure is 132/84 mm Hg; pulse rate is 82/min, rhythmic, and regular. Lungs are clear on auscultation and cardiovascular examination demonstrates scratchy and squeaking sounds at the left sternal border. Kussmaul sign is positive and ECG shows new widespread ST segment elevation and PR depression. The most likely cause for these findings in this patient is?
A 74-year-old man comes to the physician for a 6-month history of progressively worsening fatigue and shortness of breath on exertion. He immigrated to the United States 35 years ago from India. His pulse is 89/min and blood pressure is 145/60 mm Hg. Crackles are heard at the lung bases. Cardiac examination shows a grade 3/6 early diastolic murmur loudest at the third left intercostal space. Further evaluation of this patient is most likely to show which of the following?
An abnormal wave is noted on a routine ECG. The wave in question represents which of the following electrical events in the cardiac cycle?
A 27-year-old male arrives in the emergency department with a stab wound over the precordial chest wall. The patient is in distress and is cold, sweaty, and pale. Initial physical examination is significant for muffled heart sounds, distended neck veins, and a 3 cm stab wound near the left sternal border. Breath sounds are present bilaterally without evidence of tracheal deviation. Which of the following additional findings would be expected on further evaluation?
Seventy-two hours after admission for an acute myocardial infarction, a 48-year-old man develops dyspnea and a productive cough with frothy sputum. Physical examination shows coarse crackles in both lungs and a blowing, holosystolic murmur heard best at the apex. ECG shows Q waves in the anteroseptal leads. Pulmonary capillary wedge pressure is 23 mm Hg. Which of the following is the most likely cause of this patient’s current condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app