
SGLT-2 inhibitors — MCQs

A 52-year-old man comes to the physician for a routine health maintenance examination. He feels well. His blood pressure is 125/70 mm Hg. His glomerular filtration rate is calculated to be 105 mL/min/1.73 m2 and glucose clearance is calculated to be 103 mL/min. This patient is most likely being treated with which of the following agents?
A 54-year-old African American man presents to the clinic for his first annual well-check. He was unemployed for years but recently received health insurance from a new job. He reports feeling healthy and has no complaints. His blood pressure is 157/90 mmHg, pulse is 86/min, and respirations are 12/min. Routine urinalysis demonstrated a mild increase in albumin and creatinine. What medication is indicated at this time?
A 42-year-old man presents to his primary care physician for preventative care. He does not have any current complaint. His father died of diabetic nephropathy. Vital signs include a temperature of 36.7°C (98.06°F), blood pressure of 150/95 mm Hg, and pulse of 90/min. His fasting blood glucose is 159 mg/dL (on 2 occasions) and HbA1c is 8.1%. The patient is started on metformin and lifestyle modifications. 3 months later, he comes for a follow-up visit. His serum blood glucose is 370 mg/dL and HbA1C is 11%. The patient currently complains of weight loss and excessive urination. Which of the following is the optimal therapy for this patient?
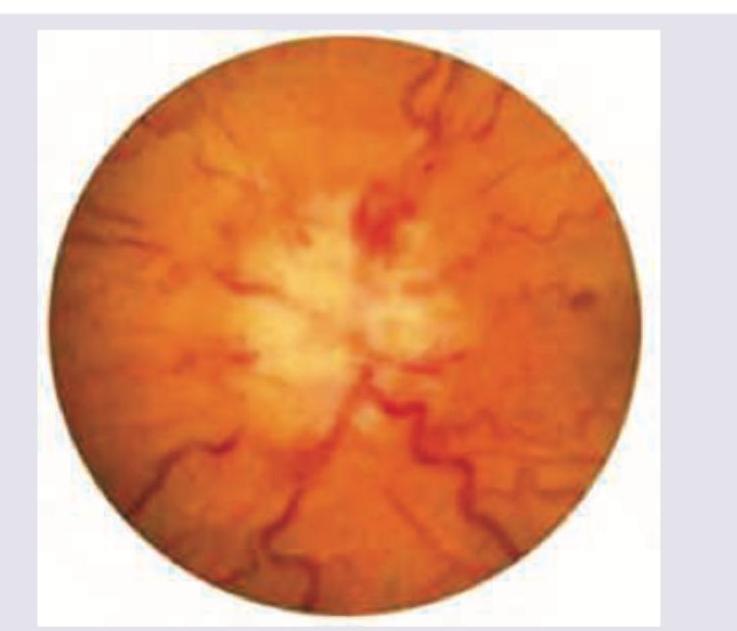
A 30-year-old obese female presents with new-onset headaches, ringing in her ears, and blurry vision. Ibuprofen and avoidance of light has not relieved her symptoms. She denies a history of recent trauma, fever, chills, and fatigue. Past medical history is significant for type 2 diabetes mellitus managed with metformin. She has had 20/20 vision her whole life and wonders if she might need to get eyeglasses. She has 2 healthy school-age children. Her temperature is 36.8°C (98.2°F), heart rate is 90/min, respiratory rate is 15/min, and blood pressure is 135/80 mm Hg. Physical exam is notable for decreased lateral eye movement, and the funduscopic findings are shown in the picture. Laboratory findings are within normal limits and brain imaging is normal. Lumbar puncture demonstrates an elevated opening pressure and normal CSF composition. Which of the following is a side effect of the medication used to treat this condition?
A 52-year-old woman makes a follow-up appointment with her primary care physician for evaluation of her diabetes medications. Specifically, she complains that she has been experiencing flushing, nausea, and palpitations after drinking a glass of wine with dinner after she started the latest regimen for her diabetes. She was warned that this was a side-effect of one of her medications but she did not understand the severity of the reaction. Given this experience, she asks to be placed on an alternative regimen that does not involve the medication that caused this reaction. Her physician therefore replaces the medication with another one that interacts with the same target though at a different binding site. Which of the following is a side-effect of the new medication?
A randomized controlled trial was initiated to evaluate a novel DPP-4 inhibitor for blood glucose management in diabetic patients. The study used a commonly prescribed sulfonylurea as the standard of care treatment. 2,000 patients were enrolled in the study with 1,000 patients in each arm. One of the primary outcomes was the development of diabetic nephropathy during treatment. This outcome occurred in 68 patients on the DPP-4 inhibitor and 134 patients on the sulfonylurea. What is the relative risk reduction (RRR) for patients using the DPP-4 inhibitor compared with the sulfonylurea?
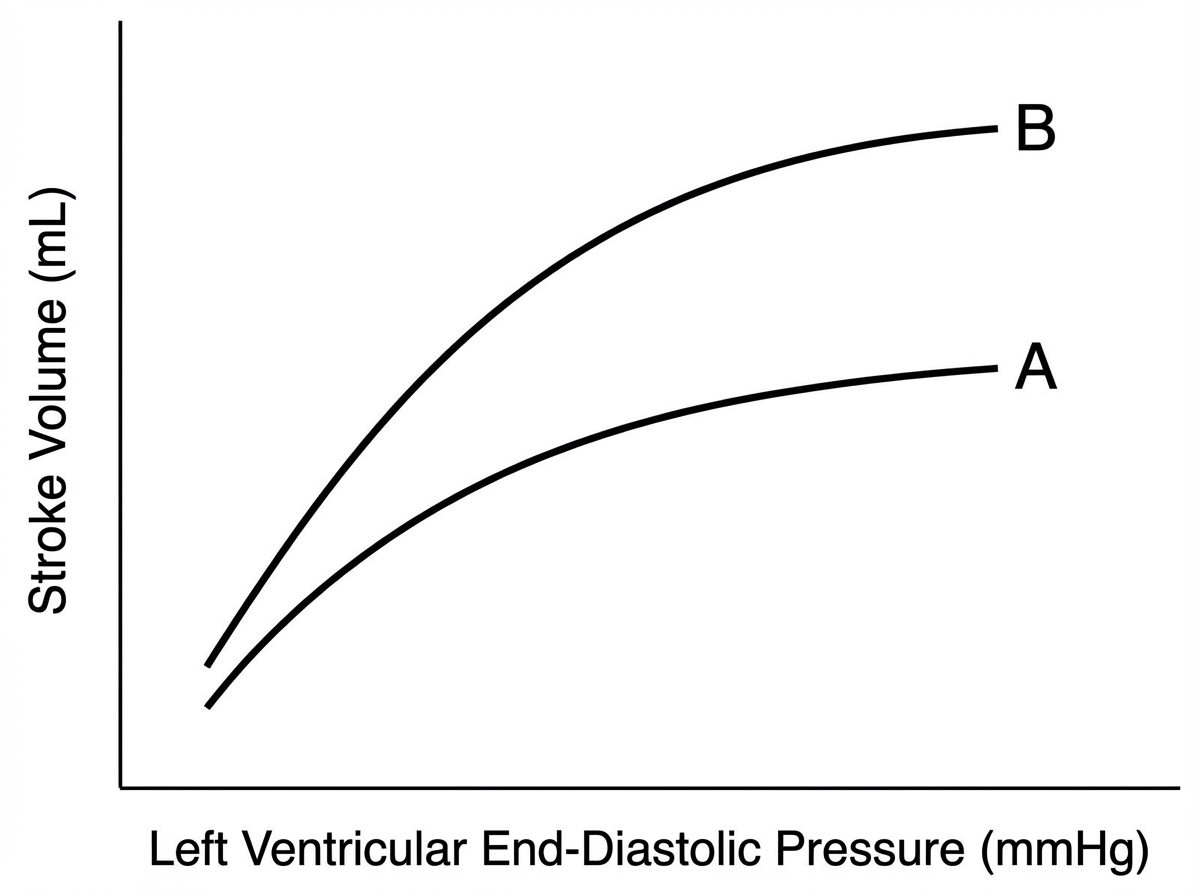
A 78-year-old male comes to the physician’s office for a routine check-up. He complains of increased lower extremity swelling, inability to climb the one flight of stairs in his home, and waking up in the middle of the night 2-3 times gasping for breath. He has had to increase the number of pillows on which he sleeps at night. These symptoms started 9 months ago and have been progressing. The doctor starts him on a medication regimen, one of which changes his Starling curve from A to B as shown in the Figure. Which of the following medications is most consistent with this mechanism of action?
A 55-year-old male is hospitalized for acute heart failure. The patient has a 20-year history of alcoholism and was diagnosed with diabetes mellitus type 2 (DM2) 5 years ago. Physical examination reveals ascites and engorged paraumbilical veins as well as 3+ pitting edema around both ankles. Liver function tests show elevations in gamma glutamyl transferase and aspartate transaminase (AST). Of the following medication, which most likely contributed to this patient's presentation?
A 63-year-old woman presents with dyspnea on exertion. She reports that she used to work in her garden without any symptoms, but recently she started to note dyspnea and fatigue after working for 20–30 minutes. She has type 2 diabetes mellitus diagnosed 2 years ago but she does not take any medications preferring natural remedies. She also has arterial hypertension and takes torsemide 20 mg daily. The weight is 88 kg and the height is 164 cm. The vital signs include: blood pressure is 140/85 mm Hg, heart rate is 90/min, respiratory rate is 14/min, and the temperature is 36.6℃ (97.9℉). Physical examination is remarkable for increased adiposity, pitting pedal edema, and present S3. Echocardiography shows a left ventricular ejection fraction of 51%. The combination of which of the following medications would be a proper addition to the patient’s therapy?
A 63-year-old African American man presents to the physician for a follow-up examination. He has a history of chronic hypertension and type 2 diabetes mellitus. He has no history of coronary artery disease. His medications include aspirin, hydrochlorothiazide, losartan, and metformin. He exercises every day and follows a healthy diet. He does not smoke. He consumes alcohol moderately. There is no history of chronic disease in the family. His blood pressure is 125/75 mm Hg, which is confirmed on a repeat measurement. His BMI is 23 kg/m2. The physical examination shows no abnormal findings. The laboratory test results show: Serum HbA1C 6.9% Total cholesterol 176 mg/dL Low-density lipoprotein (LDL-C) 105 mg/dL High-density lipoprotein (HDL-C) 35 mg/dL Triglycerides 175 mg/dL The patient's 10-year risk of cardiovascular disease (CVD) is 18.7%. Lifestyle modifications including diet and exercise have been instituted. Which of the following is the most appropriate next step in pharmacotherapy?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app