
Pharmacodynamic interaction mechanisms — MCQs

A 50-year-old woman presents with acute onset fever and chills for the past hour. She mentions earlier in the day she felt blue, so she took some St. John’s wort because she was told by a friend that it helps with depression. Past medical history is significant for hypertension, diabetes mellitus, and depression managed medically with captopril, metformin, and fluoxetine. She has no history of allergies. Her pulse is 130/min, the respiratory rate is 18/min, the blood pressure is 176/92 mm Hg, and the temperature is 38.5°C (101.3°F). On physical examination, the patient is profusely diaphoretic and extremely irritable when asked questions. Oriented x 3. The abdomen is soft and nontender with no hepatosplenomegaly. Increased bowel sounds are heard in the abdomen. Deep tendon reflexes are 3+ bilaterally and clonus is elicited. The sensation is decreased in the feet bilaterally. Mydriasis is present. Fingerstick glucose is 140 mg/dL. An ECG shows sinus tachycardia but is otherwise normal. Which of the following is the most likely cause of this patient’s condition?
A 59-year-old man is brought to the emergency department one hour after developing shortness of breath and “squeezing” chest pain that began while he was mowing the lawn. He has asthma, hypertension, and erectile dysfunction. Current medications include salmeterol, amlodipine, lisinopril, and vardenafil. His pulse is 110/min and blood pressure is 122/70 mm Hg. Physical examination shows diaphoresis. An ECG shows sinus tachycardia. Sublingual nitroglycerin is administered. Five minutes later, his pulse is 137/min and his blood pressure is 78/40 mm Hg. Which of the following is the most likely mechanism of this patient's hypotension?
A 71-year-old man presents to his oncologist with nausea. He recently underwent chemotherapy for pancreatic cancer and has developed severe intractable nausea over the past week. He vomits several times a day. His past medical history is notable for gout, osteoarthritis, and major depressive disorder. He takes allopurinol and sertraline. He has a 15-pack-year smoking history and drinks 1 glass of wine per day. His temperature is 98.6°F (37°C), blood pressure is 148/88 mmHg, pulse is 106/min, and respirations are 22/min. On exam, he is lethargic but able to answer questions appropriately. He has decreased skin turgor and dry mucous membranes. He is started on a medication to treat nausea. However, 3 days later he presents to the emergency room with fever, agitation, hypertonia, and clonus. What is the most likely mechanism of action of the drug this patient was prescribed?
A 14-year-old boy is brought to the emergency department because of a 4-hour history of vomiting, lethargy, and confusion. Three days ago, he was treated with an over-the-counter medication for fever and runny nose. He is oriented only to person. His blood pressure is 100/70 mm Hg. Examination shows bilateral optic disc swelling and hepatomegaly. His blood glucose concentration is 65 mg/dL. Toxicology screening for serum acetaminophen is negative. The over-the-counter medication that was most likely used by this patient has which of the following additional effects?
A 25-year-old woman presents to the ED with nausea, vomiting, diarrhea, abdominal pain, and hematemesis after ingesting large quantities of a drug. Which of the following pairs a drug overdose with the correct antidote for this scenario?
A 52-year-old man with a history of hypertension and hyperlipidemia comes to the physician because of a 10-month history of substernal chest pain on exertion that is relieved with rest. His pulse is 82/min and blood pressure is 145/82 mm Hg. He is prescribed a drug that acts by forming free radical nitric oxide. The patient is most likely to experience which of the following adverse effects as a result of this drug?
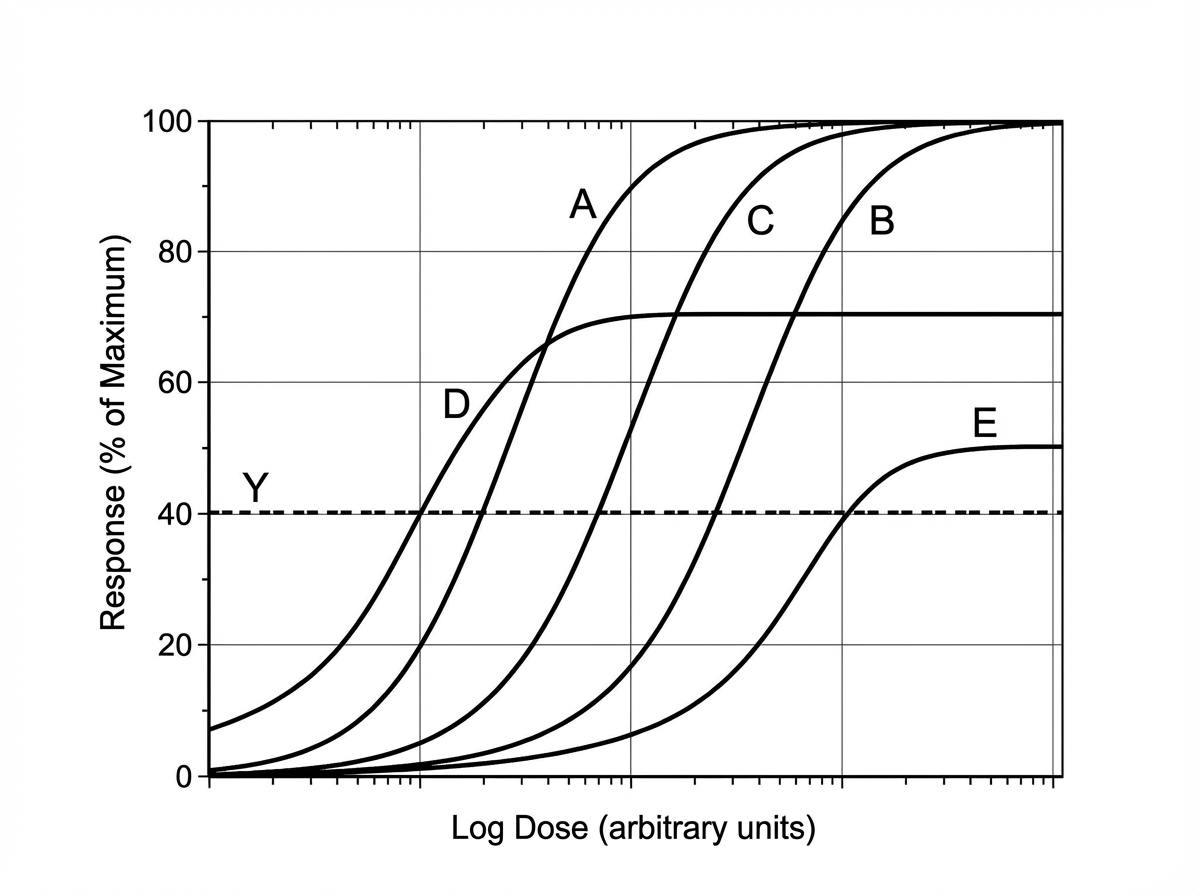
Scientists are developing a new non-steroidal anti-inflammatory drug for osteoarthritis. Their hope is that the new drug will have a higher potency but the same efficacy as ibuprofen in the hope of minimizing gastrointestinal side effects. If ibuprofen is curve C in the figure provided, which of the following would be the curve for the new drug based on the scientists’ specifications? The desired therapeutic effect in patients is represented by the dashed line Y.
A 22-year-old woman presents to the emergency department because of agitation and sweating. History shows she is currently being treated for depression with citalopram. She also takes tramadol for back pain. Her temperature is 38.6°C (101.5°F), the pulse is 108/min, the respirations are 18/min, and the blood pressure is 165/110 mm Hg. Physical examination shows hyperreflexia and mild tremors in all 4 extremities. Which of the following should be used in the next step of management for this patient?
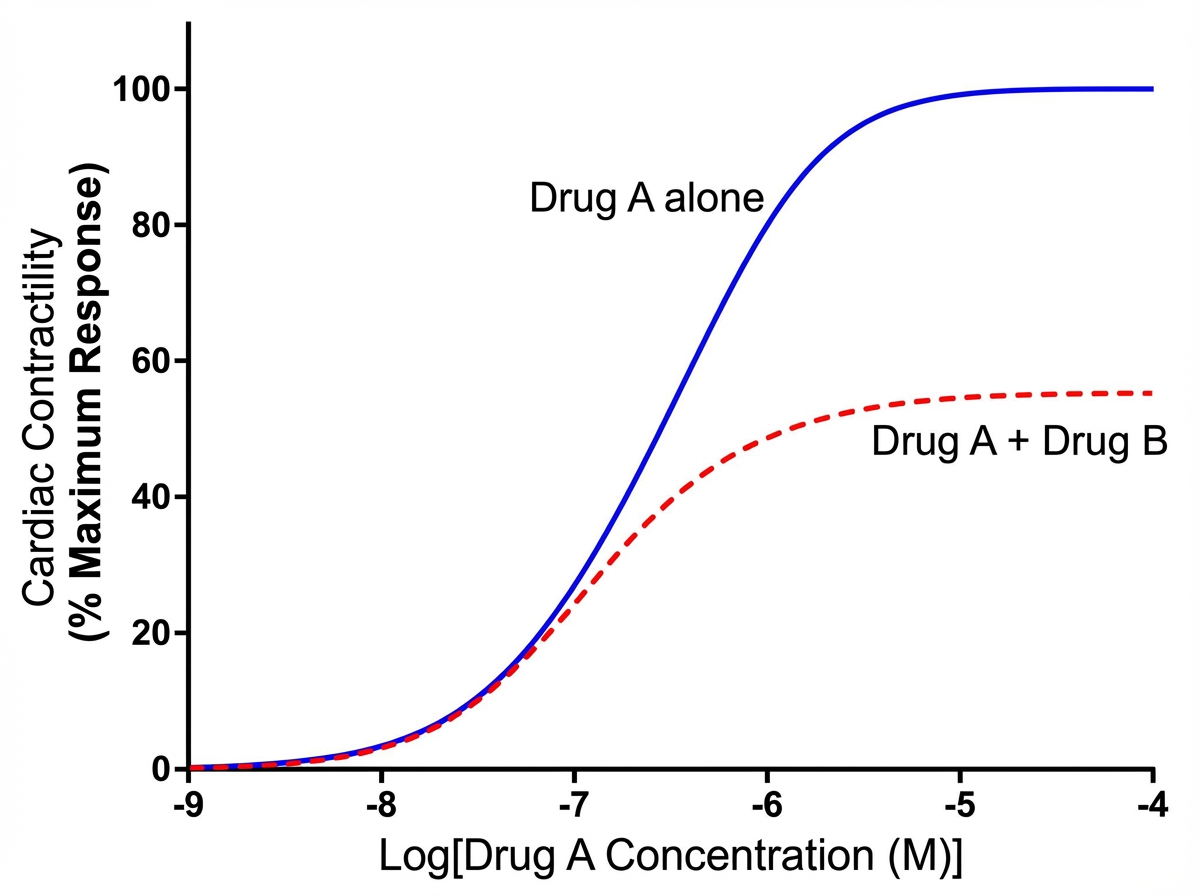
An investigator is studying the effects of different drugs on the contraction of cardiomyocytes. The myocytes are able to achieve maximal contractility with the administration of drug A. The subsequent administration of drug B produces the response depicted in the graph shown. Which of the following drugs is most likely to produce a response similar to that of drug B?
A 64-year-old man presents to the emergency department with acute onset of chest pain. He says the pain is substernal and radiates to his left arm. He has a history of hypertension, diabetes mellitus, erectile dysfunction, benign prostate hyperplasia, and panic disorder. He takes aspirin, lisinopril, metformin, sildenafil, prazosin, and citalopram. An electrocardiogram shows new ST-elevations in the lateral leads. He undergoes catherization, which reveals a complete blockage of the left circumflex artery. A stent is placed, and the patient is discharged with clopidogrel and isosorbide mononitrate. Five days later the patient presents to the emergency department complaining of fainting spells. The patient’s temperature is 97°F (37.2°C), blood pressure is 89/53 mmHg, and pulse is 90/min. Physical examination is unremarkable. An electrocardiogram reveals lateral Q waves without ST or T wave abnormalities. Which of the following is the most likely cause of the patient’s presentation?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app