
Drug interactions and adverse effects — MCQs

On this page
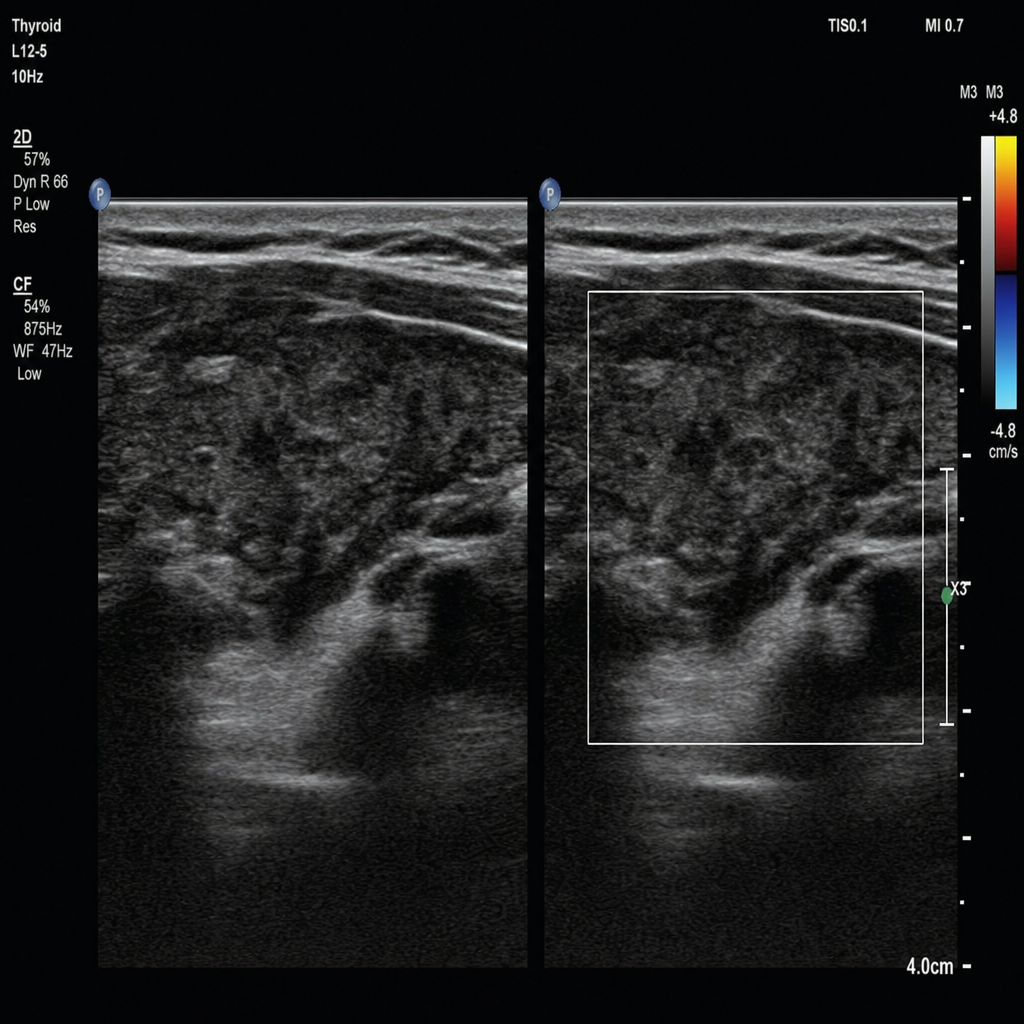
A 62-year-old man with a history of atrial fibrillation is admitted for elective cardioversion. He has been on amiodarone for rate control for the past 8 months. Laboratory results show TSH < 0.01 mIU/L, free T4 elevated, and free T3 elevated. He denies palpitations or heat intolerance. A thyroid ultrasound with color Doppler is performed and demonstrates absent vascularity within a heterogeneous gland. Which of the following best describes the underlying pathophysiology of his thyroid abnormality?
A 70-year-old man with Parkinson disease controlled on levodopa/carbidopa for 5 years develops psychotic symptoms. His neurologist considers adding an antipsychotic but is concerned about worsening parkinsonism. His family reports he has good motor control currently but the hallucinations are distressing. Evaluate the most appropriate antipsychotic choice considering the drug interaction profile.
A 35-year-old woman taking combined oral contraceptives for 2 years develops a breakthrough seizure. She is started on carbamazepine for newly diagnosed epilepsy. Four weeks later, she presents with irregular vaginal bleeding and is concerned about contraceptive failure. Apply pharmacological principles to explain the most appropriate management.
A 58-year-old man with type 2 diabetes on metformin and a recent kidney transplant on tacrolimus presents with persistent hyperglycemia. His nephrologist wants to optimize diabetic control while maintaining stable immunosuppression. His tacrolimus trough level has been stable at 8 ng/mL. Evaluate the safest approach to intensify diabetes management.
A 42-year-old woman with major depression has failed multiple SSRI trials. Her psychiatrist initiates phenelzine (MAOI). Two weeks later, she develops severe headache, diaphoresis, and hypertension (BP 210/120 mmHg) after eating at a restaurant. Which food item most likely precipitated this hypertensive crisis?
A 62-year-old man with heart failure is on digoxin, furosemide, and spironolactone. He develops acute gout and his primary care physician prescribes indomethacin. One week later, he presents with nausea, visual disturbances (yellow halos), and cardiac arrhythmias. His digoxin level is elevated at 3.2 ng/mL (therapeutic: 0.5-2.0). Analyze the most likely mechanism contributing to digoxin toxicity in this patient.
A 38-year-old woman with epilepsy well-controlled on phenytoin for 5 years presents requesting oral contraceptives. Her seizures have been absent for 3 years. She is concerned about pregnancy. What is the most appropriate counseling regarding this drug combination?
A 72-year-old woman with chronic pain on long-term oxycodone therapy develops a urinary tract infection. She is prescribed clarithromycin. Three days later, she presents to the emergency department with severe sedation, respiratory depression (respiratory rate 8/min), and pinpoint pupils. Evaluate the most appropriate immediate management considering the underlying drug interaction.
A 55-year-old man with HIV on a stable antiretroviral regimen including ritonavir presents with new-onset chest pain. Cardiac catheterization reveals significant coronary artery disease requiring stent placement. The cardiologist wants to start clopidogrel for dual antiplatelet therapy. What is the most important consideration regarding this drug combination?
A 45-year-old woman with bipolar disorder controlled on lithium presents with confusion, tremor, and ataxia. Her lithium level is 2.8 mEq/L (therapeutic: 0.6-1.2). She recently started a new medication prescribed by her primary care physician for hypertension. Which antihypertensive medication most likely caused this interaction?
Practice by Chapter
Pharmacokinetic interaction mechanisms
Practice Questions
Pharmacodynamic interaction mechanisms
Practice Questions
CYP450 inhibition and induction
Practice Questions
P-glycoprotein interactions
Practice Questions
QT prolongation and torsades de pointes
Practice Questions
Serotonin syndrome
Practice Questions
Neuroleptic malignant syndrome
Practice Questions
DRESS syndrome and severe cutaneous reactions
Practice Questions
Drug-induced liver injury
Practice Questions
Drug-induced kidney injury
Practice Questions
Drug-food interactions
Practice Questions
Polypharmacy management
Practice Questions
Pharmacovigilance principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app