
Positive inotropic agents — MCQs

An 82-year-old male with congestive heart failure experiences rapid decompensation of his condition, manifesting as worsening dyspnea, edema, and increased fatigue. Labs reveal an increase in his serum creatinine from baseline. As part of the management of this acute change, the patient is given IV dobutamine to alleviate his symptoms. Which of the following effects occur as a result of this therapy?
A 65-year-old male with a history of CHF presents to the emergency room with shortness of breath, lower leg edema, and fatigue. He is diagnosed with acute decompensated congestive heart failure, was admitted to the CCU, and treated with a medication that targets beta-1 adrenergic receptors preferentially over beta-2 adrenergic receptors. The prescribing physician explained that this medication would only be used temporarily as its efficacy decreases within 2-3 days due to receptor downregulation. Which of the following was prescribed?
A 25-year-old man is admitted to the intensive care unit with confusion and severe dyspnea at rest which started 3 hours ago. The symptoms worsen when the patient lies down and improve in the sitting position. The patient has a history of cocaine abuse. The patient's blood pressure is 75/50 mm Hg, the heart rate is 95/min, the respiratory rate is 22/min, the temperature is 36.5℃ (97.7℉), and the SpO2 is 89% on room air. On physical examination, there is peripheral cyanosis with pallor, coldness of the extremities, diaphoresis, and marked peripheral veins distension. Lung auscultation reveals bilateral absence of the lung sounds over the lower lobes and widespread rales over the other lung fields. On cardiac auscultation, there is a protodiastolic gallop and S2 accentuation best heard in the second intercostal space at the left sternal border. Abdominal palpation shows signs of intraperitoneal fluid accumulation and hepatomegaly. Considering the low cardiac output, milrinone is administered as an inotropic agent. What is the most likely side effect which can result from administration of milrinone?
A 77-year-old man with refractory shock has been under treatment in an intensive care unit for last 7 days. Despite the best possible management by the team of physicians and intensivists, he fails to show improvement. After discussion with his relatives and obtaining informed consent from them, the team administers to him a novel drug, an adrenergic agonist that produces positive chronotropic effects and inotropic effects and stimulates the release of renin from the kidneys. The drug does not have any other adrenergic effects. Which of the following second messengers is most likely to be responsible for the actions of the novel drug?
An 82-year-old male with a history of congestive heart failure presented with new-onset atrial fibrillation. He was initially started on carvedilol, but he now requires an additional agent for rate control. He is started on a medicine and is warned by his physician of the following potential side effects associated with this therapy: nausea, vomiting, confusion, blurry yellow vision, electrolyte abnormalities, and potentially fatal arrhythmia. Which of the following is most likely to increase this patient's susceptibility to the toxic effects associated with this medication?
A previously healthy 52-year-old woman comes to the physician because of a 3-month history of chest pain on exertion. She takes no medications. Cardiopulmonary examination shows no abnormalities. Cardiac stress ECG shows inducible ST-segment depressions in the precordial leads that coincide with the patient's report of chest pain and resolve upon cessation of exercise. Pharmacotherapy with verapamil is initiated. This drug is most likely to have which of the following sets of effects? $$$ End-diastolic volume (EDV) %%% Blood pressure (BP) %%% Contractility %%% Heart rate (HR) $$$
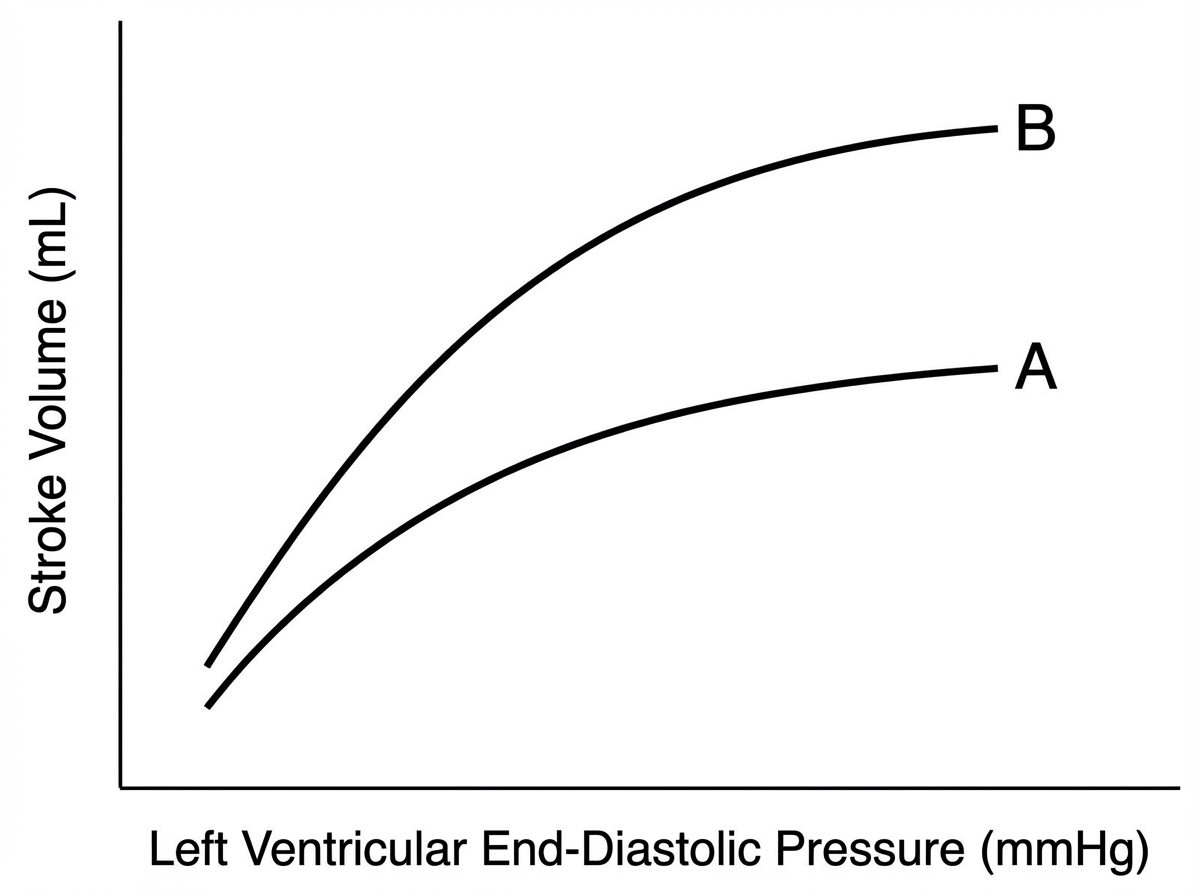
A 78-year-old male comes to the physician’s office for a routine check-up. He complains of increased lower extremity swelling, inability to climb the one flight of stairs in his home, and waking up in the middle of the night 2-3 times gasping for breath. He has had to increase the number of pillows on which he sleeps at night. These symptoms started 9 months ago and have been progressing. The doctor starts him on a medication regimen, one of which changes his Starling curve from A to B as shown in the Figure. Which of the following medications is most consistent with this mechanism of action?
A 63-year-old woman presents with dyspnea on exertion. She reports that she used to work in her garden without any symptoms, but recently she started to note dyspnea and fatigue after working for 20–30 minutes. She has type 2 diabetes mellitus diagnosed 2 years ago but she does not take any medications preferring natural remedies. She also has arterial hypertension and takes torsemide 20 mg daily. The weight is 88 kg and the height is 164 cm. The vital signs include: blood pressure is 140/85 mm Hg, heart rate is 90/min, respiratory rate is 14/min, and the temperature is 36.6℃ (97.9℉). Physical examination is remarkable for increased adiposity, pitting pedal edema, and present S3. Echocardiography shows a left ventricular ejection fraction of 51%. The combination of which of the following medications would be a proper addition to the patient’s therapy?
A 55-year-old male is hospitalized for acute heart failure. The patient has a 20-year history of alcoholism and was diagnosed with diabetes mellitus type 2 (DM2) 5 years ago. Physical examination reveals ascites and engorged paraumbilical veins as well as 3+ pitting edema around both ankles. Liver function tests show elevations in gamma glutamyl transferase and aspartate transaminase (AST). Of the following medication, which most likely contributed to this patient's presentation?
A 39-year-old man comes to the physician because of a 3-month history of fatigue, decreased sexual desire, and difficulty achieving an erection. He has no past medical history except for a traumatic brain injury he sustained in a motor vehicle accident 4 months ago. At that time, neuroimaging studies showed no abnormalities. Physical examination shows bilateral gynecomastia and a thin white nipple discharge. Decreased production of which of the following is the most likely underlying cause of this patient's current condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app