
Autonomic/CV Drugs — MCQs

On this page
A 53-year-old woman comes to the physician for a follow-up examination. One month ago, she was diagnosed with carcinoma of the left breast. She underwent a lumpectomy for a 2.1-cm mass and sentinel lymph node biopsy 2 weeks ago. The biopsy of the breast mass showed margin-free invasive ductal carcinoma; immunohistochemistry showed the carcinoma is estrogen-receptor and progesterone-receptor negative, and HER2-receptor positive. The lymph node biopsy was negative for metastases. Examination shows a healing surgical incision over the left breast. There is no palpable axillary lymphadenopathy. Her physician decides to initiate treatment with appropriate pharmacotherapy. Which of the following is the most appropriate next step in management?
Several patients at a local US hospital present with chronic secretory diarrhea. Although there are multiple potential causes of diarrhea present in these patients, which of the following is most likely the common cause of their chronic secretory diarrhea?
A 71-year-old man presents to the clinic with complaints of right wrist pain for 2 days. On examination, redness and swelling were noted on the dorsal aspect of his right wrist. He had pain with extreme range of motion of the wrist. His history includes 2 hip replacements, 2 previous episodes of gout in both first metatarsophalangeal joints, and hypertension. Two days later, the swelling had increased in the dorsal aspect of his right wrist and hand. Wrist flexion was limited to 80% with severe pain. The pain was present on palpation of the scaphoid bone. Due to the suspicion of fracture, the patient was referred to his general practitioner for radiographs. These findings were consistent with gouty arthritis. What is the most likely cytokine involved in this process?
A 23-year-old man comes to the physician because of recurrent episodes of chest pain, shortness of breath, palpitations, and a sensation of choking. The symptoms usually resolve with deep breathing exercises after about 5 minutes. He now avoids going to his graduate school classes because he is worried about having another episode. Physical examination is unremarkable. Treatment with lorazepam is initiated. The concurrent intake of which of the following drugs should be avoided in this patient?
A researcher is studying how arachidonic acid metabolites mediate the inflammatory response in rats. She has developed multiple enzyme inhibitors that specifically target individual proteins in the arachidonic acid pathway. She injects these inhibitors in rats who have been exposed to common bacterial pathogens and analyzes their downstream effects. In one of her experiments, she injects a leukotriene B4 inhibitor into a rat and observes an abnormal cell response. Which of the following interleukins would most closely restore the function of one of the missing products?
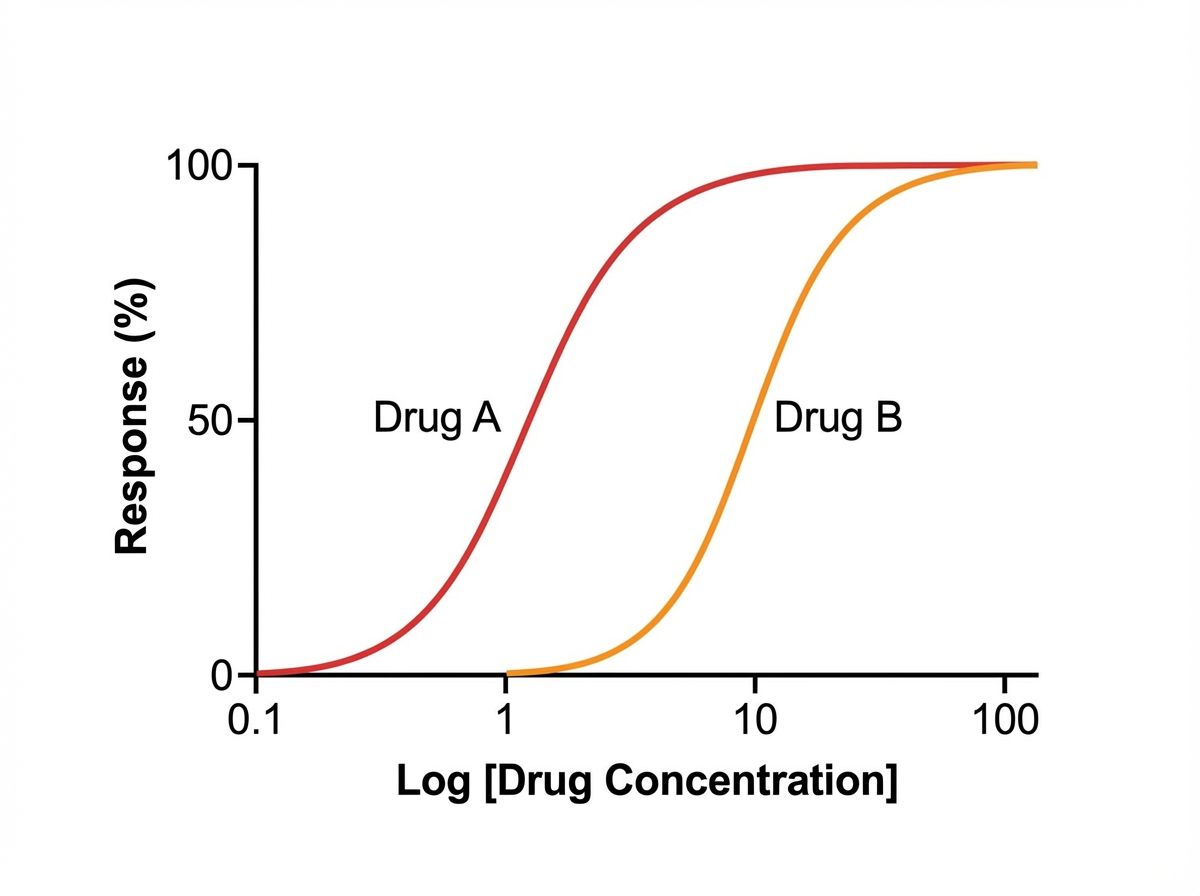
A student is reviewing the various effects that can be plotted on a dose-response curve. He has observed that certain drugs can work as an agonist and an antagonist at a particular site. He has plotted a particular graph (as shown below) and is checking for other responses that can be measured on the same graph. He learned that drug B is a competitive antagonist of drug A. Drug B reduces the potency of drug A when combined in the same solution; however, if additional drug A is added to the solution, the original Emax of drug A is restored. He wishes to plot another curve for drug C. He learns that drug C works on the same molecules as drugs A and B, but drug C reduces the maximal efficacy (Emax) of drug A significantly when combined with drug A. Which of the following best describes drug C?
An obese, 66-year-old woman comes to the physician for a routine health maintenance examination. She feels well but is unhappy about being overweight. She reports that she feels out of breath when walking for more than one block and while climbing stairs. She has tried to lose weight for several years without success. She goes for a walk 3 times a week but she has difficulty following a low-calorie diet. During the past 12 months, she has had two urinary tract infections that were treated with fosfomycin. She has type 2 diabetes mellitus and osteoarthritis. Her only current medication is metformin. She has never smoked. She is 160 cm (5 ft 3 in) tall and weighs 100 kg (220 lb); BMI is 39.1 kg/m2. Vital signs are within normal limits. Physical examination shows cracking in both knees on passive movement. The remainder of the examination shows no abnormalities. Serum studies show an HbA1c of 9.5%, and a fasting serum glucose concentration of 158 mg/dL. An ECG shows no abnormalities. Which of the following is the most appropriate pharmacotherapy?
A 65-year-old male with a history of CHF presents to the emergency room with shortness of breath, lower leg edema, and fatigue. He is diagnosed with acute decompensated congestive heart failure, was admitted to the CCU, and treated with a medication that targets beta-1 adrenergic receptors preferentially over beta-2 adrenergic receptors. The prescribing physician explained that this medication would only be used temporarily as its efficacy decreases within 2-3 days due to receptor downregulation. Which of the following was prescribed?
A 42-year-old male presents to the emergency department due to severe headaches and palpitations. He has had previous episodes of sweating and headache, but this episode was particularly disabling. Upon presentation, he appears pale and diaphoretic. His temperature is 99.3°F (37.4°C), blood pressure is 162/118 mmHg, pulse is 87/min, and respirations are 20/min. Based on clinical suspicion, an abdominal CT scan is obtained, which shows a retroperitoneal mass. This patient's increased heart rate is most likely due to a change in activity of which of the following channels?
A 28-year-old woman comes to the emergency department because of increasing abdominal pain for 2 days. The pain is diffuse and constant, and she describes it as 7 out of 10 in intensity. She has also had numbness in her lower extremities for 12 hours. She has type 1 diabetes mellitus, migraine with aura, and essential tremor. She appears uncomfortable. She is oriented to place and person only. Her temperature is 37°C (98.6°F), pulse is 123/min, and blood pressure is 140/70 mm Hg. Examination shows a distended abdomen with no tenderness to palpation. Bowel sounds are decreased. Muscle strength and sensation is decreased in the lower extremities. There is a tremor of the right upper extremity. Urinalysis shows elevated levels of aminolevulinic acid and porphobilinogen. Which of the following is the most likely cause of this patient's symptoms?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app