
Autonomic/CV Drugs — MCQs

On this page
A 70-year-old man is brought to the emergency department with complaints of chest pain for the last 2 hours. He had been discharged from the hospital 10 days ago when he was admitted for acute myocardial infarction. It was successfully treated with percutaneous coronary intervention. During the physical exam, the patient prefers to hunch forwards as this decreases his chest pain. He says the pain is in the middle of the chest and radiates to his back. Despite feeling unwell, the patient denies any palpitations or shortness of breath. Vitals signs include: pulse 90/min, respiratory rate 20/min, blood pressure 134/82 mm Hg, and temperature 36.8°C (98.2°F). The patient is visibly distressed and is taking shallow breaths because deeper breaths worsen his chest pain. An ECG shows diffuse ST elevations. Which of the following should be administered to this patient?
A 69-year-old man comes to his cardiologist for a follow-up visit. He is being considered for a new drug therapy that works by modulating certain proteins released from the heart in patients with heart failure. A drug called candoxatril is being investigated for its ability to inhibit the action of an endopeptidase that breaks down a vasodilatory mediator released from the heart, as well as, endothelin and bradykinin. This mediator is known to promote the excretion of sodium from the body and improve the ejection fraction. One of its side effects is its ability to increase angiotensin II levels which causes harm to patients with heart failure. Therefore, to improve efficacy and reduce its adverse effects, candoxatril has to be used in conjunction with angiotensin receptor blockers. Which of the following is most likely to increase as a result of this drug regimen?
A 25-year-old woman is rushed to the emergency department after she was found unconscious in a house fire. She has no previous medical history available. At the hospital, the vital signs include: blood pressure 110/70 mm Hg, temperature 36.0°C (97.0°F), and heart rate 76/min with oxygen saturation 99% on room air. On physical exam she is unconscious. There are superficial burns on her hands and parts of her face. Her face and clothes are blackened with soot. What is the 1st best step while treating this patient?
A 59-year-old male presents to the emergency room complaining of substernal chest pain. He reports a three-hour history of dull substernal chest pain that radiates into his left arm and jaw. He has experienced similar chest pain before that was brought on with exertion, but this pain is more severe and occurred with rest. His past medical history includes gout, hypertension, diabetes mellitus, and hyperlipidemia. An EKG demonstrates ST segment depression. Serum troponin is elevated. In addition to aspirin, oxygen, and morphine, he is started on a sublingual medication. What is the main physiologic effect of this medication?
A 17-year-old male presents with altered mental status. He was recently admitted to the hospital due to a tibial fracture suffered while playing soccer. His nurse states that he is difficult to arouse. His temperature is 98.6 deg F (37 deg C), blood pressure is 130/80 mm Hg, pulse is 60/min, and respirations are 6/min. Exam is notable for pinpoint pupils and significant lethargy. Which of the following describes the mechanism of action of the drug likely causing this patient's altered mental status?
A hospitalized 70-year-old woman, who recently underwent orthopedic surgery, develops severe thrombocytopenia of 40,000/mm3 during her 7th day of hospitalization. She has no other symptoms and has no relevant medical history. All of the appropriate post-surgery prophylactic measures had been taken. Her labs from the 7th day of hospitalization are shown here: The complete blood count results are as follows: Hemoglobin 13 g/dL Hematocrit 38% Leukocyte count 8,000/mm3 Neutrophils 54% Bands 3% Eosinophils 1% Basophils 0% Lymphocytes 33% Monocytes 7% Platelet count 40,000/mm3 The coagulation tests are as follows: Partial thromboplastin time (activated) 85 seconds Prothrombin time 63 seconds Reticulocyte count 1.2% Thrombin time < 2 seconds deviation from control The lab results from previous days were within normal limits. What is the most likely cause of the thrombocytopenia?
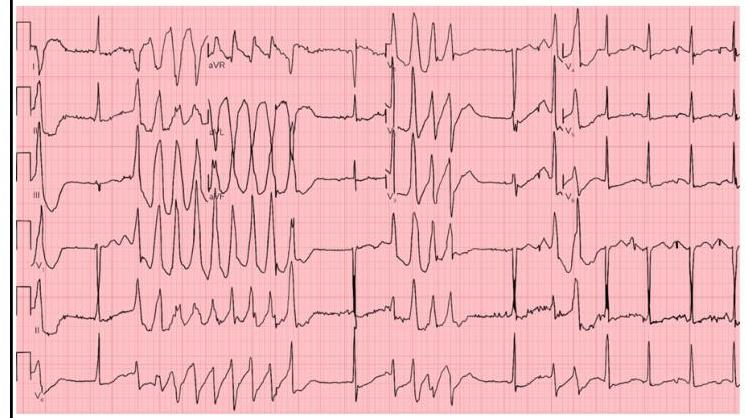
A 53-year-old man with obesity and heart disease presents to your outpatient clinic with complaints of orthopnea, significant dyspnea on minimal exertion, nausea, vomiting, and diarrhea. He says that his old doctor gave him "some pills" that he takes in varying amounts every morning. Physical exam is significant for a severely displaced point of maximal impulse, bilateral rales in the lower lung fields, an S3 gallop, and hepatomegaly. You decide to perform an EKG (shown in figure A). Suddenly, his rhythm changes to ventricular tachycardia followed by ventricular fibrillation, and he syncopizes and expires despite resuscitative efforts. High levels of which medication are most likely responsible?
Four days after admission to the hospital for anorexia nervosa, a 20-year-old woman has new-onset palpitations and paresthesias in all four limbs. Prior to admission, she was found unconscious by her parents on the floor of a residential treatment center. The patient was started on a trial of nutritional rehabilitation upon arrival to the hospital. Her temperature is 36°C (96.8°F), pulse is 47/min, and blood pressure is 90/60 mmHg. She is 160 cm tall and weighs 35 kg; BMI is 14 kg/m2. The patient appears emaciated. Examination shows lower leg edema. A 2/6 holosystolic murmur is heard over the 5th intercostal space at the midclavicular line. An ECG shows intermittent supraventricular tachycardia and QTc prolongation. Serum studies show: Day 2 Day 4 Potassium (mEq/L) 3.5 2.7 Calcium (mg/dL) 8.5 7.8 Magnesium (mEq/L) 1.2 0.5 Phosphorus (mg/dL) 3.6 1.5 Which of the following is the most likely underlying cause of this patient's condition?
A 23-year-old patient with a past medical history of anxiety and appropriately treated schizophrenia presents to the emergency department for a first time seizure. The patient was at home eating dinner when he began moving abnormally and did not respond to his mother, prompting her to bring him in. His symptoms persisted in the emergency department and were successfully treated with diazepam. The patient is discharged and scheduled for a follow up appointment with neurology the next day for treatment. The patient returns to his neurologist 1 month later for a checkup. Physical exam is notable for carpopedal spasm when his blood pressure is being taken. Cranial nerves II-XII are grossly intact and his gait is stable. Which of the following is the most likely explanation of this patient's current presentation?
A 72-year-old man presents to his primary care provider to discuss the frequency with which he wakes up at night to urinate. He avoids drinking liquids at night, but the symptoms have progressively worsened. The medical history is significant for hypertension and hyperlipidemia. He takes lisinopril, atorvastatin, and a multivitamin every day. Today, the vital signs include: blood pressure 120/80 mm Hg, heart rate 90/min, respiratory rate 17/min, and temperature 37.0°C (98.6°F). On physical examination, he appears tired. The heart has a regular rate and rhythm and the lungs are clear to auscultation bilaterally. A bedside bladder ultrasound reveals a full bladder. A digital rectal exam reveals an enlarged and symmetric prostate free of nodules, that is consistent with benign prostatic enlargement. He also has a history of symptomatic hypotension with several episodes of syncope in the past. The patient declines a prostate biopsy that would provide a definitive diagnosis and requests less invasive treatment. Which of the following is recommended to treat this patient’s enlarged prostate?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app