
Autonomic/CV Drugs — MCQs

On this page
A 27-year-old woman develops progressive difficulty breathing after a long day of chores in a dusty house. These chores included brushing the family dog, vacuuming, dusting, and sweeping. She occasionally gets these episodes once or twice a year and has her medication on hand. Her symptoms are reversed by inhaling a β2-adrenergic receptor agonist. Which of the following chemical mediators is responsible for this patient’s breathing difficulties?
A 65-year-old man comes to the physician because of a 2-week history of chest pain that begins after walking at a brisk pace for 2 blocks. The pain does not radiate anywhere and is hard to localize. He has had similar episodes in the past 6 months and was prescribed sublingual nitroglycerin, which helps relieve the pain. The patient has hypertension and type 2 diabetes mellitus. He takes lisinopril and metformin daily. He appears well. His temperature is 37°C (98.6°F), pulse is 75/min, and blood pressure is 145/90 mm Hg. Examination shows a regular heart rhythm. S1 and S2 are normal. The lungs are clear to auscultation. There is no peripheral edema. Which of the following is the most likely explanation for the improvement of this patient's chest pain?
A 55-year-old male is started on nitrate therapy for treatment of stable angina. He experiences significant and immediate relief of his symptoms within minutes of starting therapy. Approximately 48 hours after initiating this new medication, he notes return of chest pain and pressure with exertion that no longer responds to continued nitrate use. Which of the following 24-hour dosing schedules would most likely explain this patient's response to nitrate treatment?
A 51-year-old male presents to his primary care provider for a normal check-up. He reports that he “hasn’t felt like himself” recently. He describes feeling down for the past 8 months since his mother passed away. He has had trouble sleeping and has unintentionally lost 15 pounds. He feels guilty about his mother’s death but cannot articulate why. His performance at work has declined and he has stopped running, an activity he used to enjoy. He has not thought about hurting himself or others. Of note, he also complains of numbness in his feet and fingers and inability to maintain an erection. His past medical history is notable for diabetes. He is on metformin. His temperature is 98.6°F (37°C), blood pressure is 125/65 mmHg, pulse is 90/min, and respirations are 16/min. On exam, he is alert and oriented with intact memory and normal speech. He appears tired with a somewhat flattened affect. The best medication for this patient inhibits which of the following processes?
Ten days after starting a new medication, a 60-year-old man is brought to the emergency department after a 3-minute episode of myoclonic jerking movements and urinary incontinence. After regaining consciousness, the patient had no recollection of what happened and seemed confused. He has bipolar disorder, which has been controlled with maintenance therapy for the past 15 years. Physical examination shows dry oral mucosa, muscle fasciculations, and bilateral hand tremors. His speech is slow, and he is disoriented. Which of the following drugs most likely precipitated this patient's current condition?
A 32-year-old woman is found unconscious on the office floor just before lunch by her colleagues. She had previously instructed them on the location of an emergency kit in case this ever happened so they are able to successfully inject her with the substance inside. Her past medical history is significant for type 1 diabetes for which she takes long acting insulin as well as periprandial rapid acting insulin injections. She has previously been found unconscious once before when she forgot to eat breakfast. The substance inside the emergency kit most likely has which of the following properties.
Following gastric surgery, a 45-year-old woman complains of severe nausea and vomiting on the 2nd postoperative day. On physical examination, her vitals are stable and examination of the abdomen reveals no significant abnormality. The patient is already receiving a maximum dosage of ondansetron. Metoclopramide is given, and she experiences significant relief from nausea and vomiting. Which of the following best explains the mechanism of action of this drug?
A 23-year-old man is brought to the emergency department by ambulance following a motor vehicle accident. He was pinned between 2 cars for several hours. The patient has a history of asthma. He uses an albuterol inhaler intermittently. The patient was not the driver, and admits to having a few beers at a party prior to the accident. His vitals in the ambulance are stable. Upon presentation to the emergency department, the patient is immediately brought to the operating room for evaluation and surgical intervention. It is determined that the patient’s right leg has a Gustilo IIIC injury in the mid-shaft of the tibia with a severely comminuted fracture. The patient’s left leg suffered a similar injury but with damage to the peroneal nerve. The anesthesiologist begins to induce anesthesia. Which of the following agents would be contraindicated in this patient?
An otherwise healthy 76-year-old man is brought to the physician because of poor sleep for the past several years. Every night he has been sleeping less and taking longer to fall asleep. During the day, he feels tired and has low energy and difficulty concentrating. Sleep hygiene and relaxation techniques have failed to improve his sleep. He would like to start a short-term pharmacological therapy trial but does not want a drug that makes him drowsy during the day. Which of the following is the most appropriate pharmacotherapy for this patient?
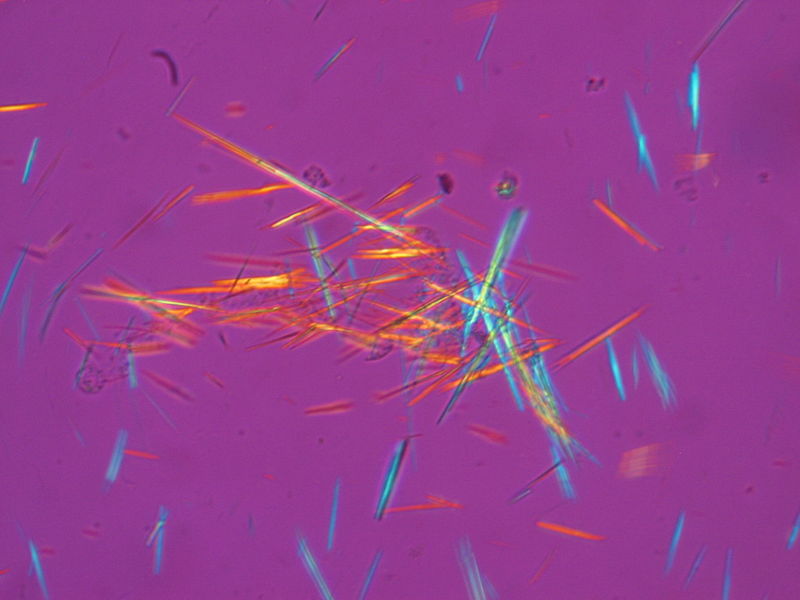
A 57-year-old man is brought to the emergency department for worsening pain and swelling of his left ankle for the past 2 hours. The pain is severe and awakened him from sleep. He has hypertension and hyperlipidemia. Current medications include hydrochlorothiazide and pravastatin. His temperature is 37.8°C (100.1°F), pulse is 105/min, and blood pressure is 148/96 mm Hg. Examination shows exquisite tenderness, erythema, and edema of the left ankle; active and passive range of motion is limited by pain. Arthrocentesis of the ankle joint yields cloudy fluid with a leukocyte count of 19,500/mm3 (80% segmented neutrophils). Gram stain is negative. A photomicrograph of the joint fluid aspirate under polarized light is shown. Which of the following is the most appropriate pharmacotherapy?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app