
Autonomic/CV Drugs — MCQs

On this page
An investigator is comparing the risk of adverse effects among various antiarrhythmic medications. One of the drugs being studied primarily acts by blocking the outward flow of K+ during myocyte repolarization. Further investigation shows that the use of this drug is associated with a lower rate of ventricular tachycardia, ventricular fibrillation, and torsades de pointes when compared to similar drugs. Which of the following drugs is most likely being studied?
A 38-year-old man presents to his primary care provider for abdominal pain. He reports that he has had a dull, burning pain for several months that has progressively gotten worse. He also notes a weight loss of about five pounds over that time frame. The patient endorses nausea and feels that the pain is worse after meals, but he denies any vomiting or diarrhea. He has a past medical history of hypertension, and he reports that he has been under an unusual amount of stress since losing his job as a construction worker. His home medications include enalapril and daily ibuprofen, which he takes for lower back pain he developed at his job. The patient drinks 1-2 beers with dinner and has a 25-pack-year smoking history. His family history is significant for colorectal cancer in his father and leukemia in his grandmother. On physical exam, the patient is moderately tender to palpation in the epigastrium. A fecal occult test is positive for blood in the stool. Which of the following in the patient’s history is most likely causing this condition?
A 26-year-old man being treated for major depressive disorder returns to his psychiatrist complaining that he has grown weary of the sexual side effects. Which other medication used to treat major depressive disorder may be appropriate as a stand-alone or add-on therapy?
A 44-year-old man presents for a checkup. The patient says he has to urinate quite frequently but denies any dysuria or pain on urination. Past medical history is significant for diabetes mellitus type 2 and hypertension, both managed medically, as well as a chronic mild cough for the past several years. Current medications are metformin, aspirin, rosuvastatin, captopril, and furosemide. His vital signs are an irregular pulse of 74/min, a respiratory rate of 14/min, a blood pressure of 130/80 mm Hg, and a temperature of 36.7°C (98.0°F). His BMI is 32 kg/m2. On physical examination, there are visible jugular pulsations present in the neck bilaterally. Laboratory findings are significant for the following: Glycated Hemoglobin (Hb A1c) 7.5% Fasting Blood Glucose 120 mg/dL Serum Electrolytes Sodium 138 mEq/L Potassium 3.9 mEq/L Chloride 101 mEq/L Serum Creatinine 1.3 mg/dL Blood Urea Nitrogen 18 mg/dL Which of the following is the next best step in the management of this patient?
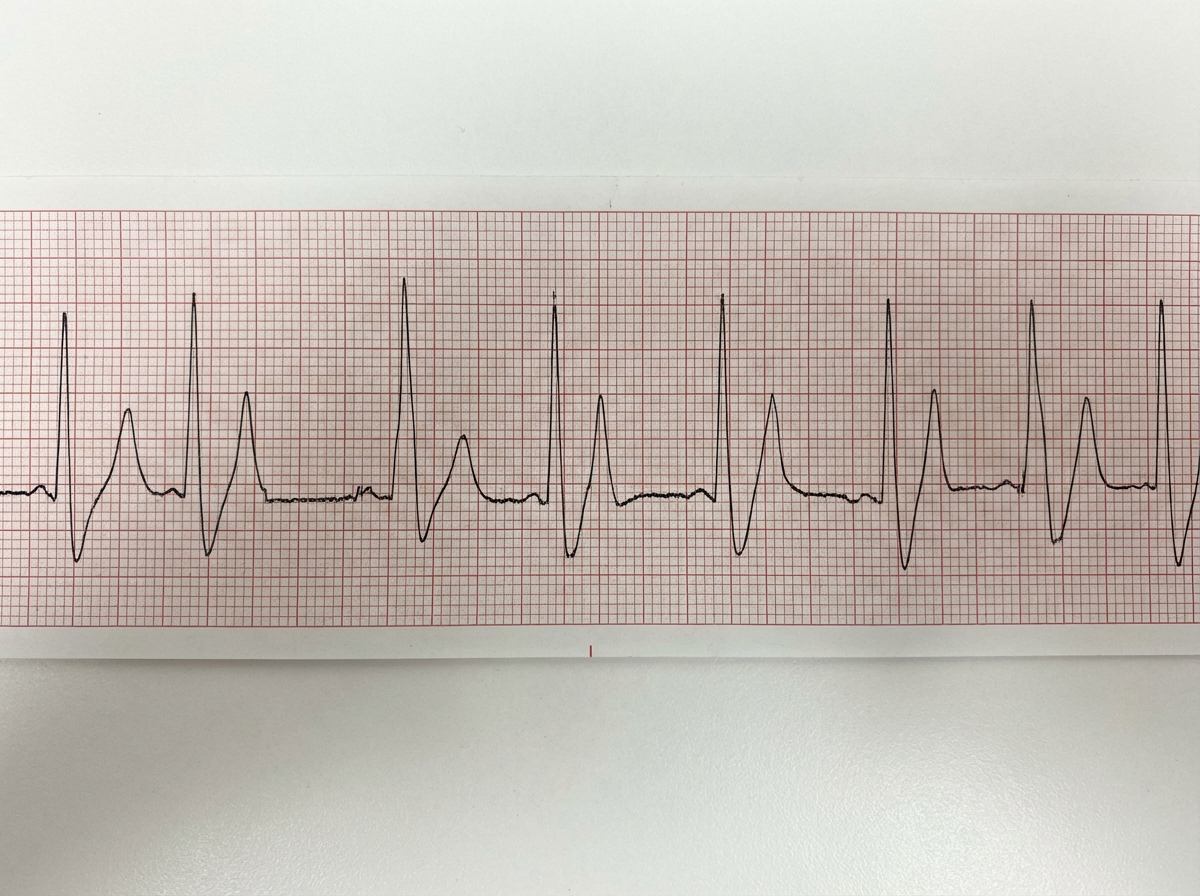
A 25-year-old male is brought into the emergency department by emergency medical services. The patient has a history of bipolar disease complicated by polysubstance use. He was found down in his apartment at the bottom of a staircase lying on his left arm. He was last seen several hours earlier by his roommate. He is disoriented and unable to answer any questions, but is breathing on his own. His vitals are HR 55, T 96.5, RR 18, BP 110/75. You decide to obtain an EKG as shown in Figure 1. What is the next best step in the treatment of this patient?
A 19-year-old South Asian male presents to the family physician concerned that he is beginning to go bald. He is especially troubled because his father and grandfather "went completely bald by the age of 25," and he is willing to try anything to prevent his hair loss. The family physician prescribes a medication that prevents the conversion of testosterone to dihydrotestosterone. Which of the following enzymes is inhibited by this medication?
A 72-year-old Caucasian woman presents with three months of progressive central vision loss accompanied by wavy distortions in her vision. She has hypertension controlled with metoprolol but has no other past medical history. Based on this clinical history she is treated with intravitreal injections of a medication. What is the mechanism of action of the treatment most likely used in this case?
A 51-year-old woman comes to the physician because of daytime sleepiness and dry mouth for one month. She says her sleepiness is due to getting up to urinate several times each night. She noticed increased thirst about a month ago and now drinks up to 20 cups of water daily. She does not feel a sudden urge prior to urinating and has not had dysuria. She has a history of multiple urinary tract infections and head trauma following a suicide attempt 3 months ago. She has bipolar I disorder and hypertension. She has smoked one pack of cigarettes daily for 25 years. Examination shows poor skin turgor. Mucous membranes are dry. Expiratory wheezes are heard over both lung fields. There is no suprapubic tenderness. She describes her mood as "good" and her affect is appropriate. Neurologic examination shows tremor in both hands. Laboratory studies show a serum sodium of 151 mEq/L. Urine osmolality is 124 mOsm/kg H2O. Which of the following is the most likely explanation for this patient's symptoms?
A scientist is studying mechanisms by which cancer drugs work to kill tumor cells. She is working to optimize the function of a drug class in order to reduce toxicity and increase potency for the target. After synthesizing a variety of analogs for the drug class, she tests these new pharmacologic compounds against a panel of potential targets. Assay results show that there is significant binding to a clustered group of proteins. Upon examining these proteins, she finds that the proteins add a phosphate group to an aromatic amino acid sidechain. Which of the following disorders would most likely be treated by this drug class?
Five days after undergoing an open colectomy and temporary colostomy for colon cancer, a 73-year-old man develops severe pain and swelling of the left calf. He was diagnosed with colon cancer 3 months ago. He has hypothyroidism and hypertension. His father died of colon cancer at the age of 68. He does not smoke. Prior to admission, his medications included levothyroxine, amlodipine, and carvedilol. Since the surgery, he has also been receiving unfractionated heparin, morphine, and piperacillin-tazobactam. He is 172 cm (5 ft 8 in) tall and weighs 101 kg (223 lb); BMI is 34.1 kg/m2. He appears uncomfortable. His temperature is 38.1°C (100.6°F), pulse is 103/min, and blood pressure is 128/92 mm Hg. Examination shows multiple necrotic lesions over bilateral thighs. The left calf is erythematous, tender, and swollen. Dorsiflexion of the left foot elicits pain behind the knee. The abdomen is soft and nontender. There is a healing midline incision and the colostomy is healthy and functioning. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 13.6 g/dL Leukocyte count 12,100/mm3 Platelet count 78,000/mm3 Prothrombin time 18 seconds (INR = 1.1) Activated partial thromboplastin time 46 seconds Serum Na+ 138 mEq/L Cl- 103 mEq/L K+ 4.1 mEq/L Urea nitrogen 18 mg/dL Glucose 101 mg/dL Creatinine 1.1 mg/dL Which of the following is the most appropriate next step in management?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app