
Autonomic/CV Drugs — MCQs

On this page
A 24-year-old woman comes to the physician because of bothersome hair growth on her face and abdomen over the past 8 years. She does not take any medications. She is 163 cm (5 ft 4 in) tall and weighs 85 kg (187 lb); BMI is 32 kg/m2. Physical examination shows coarse dark hair on the upper lip and periumbilical and periareolar skin. Her external genitalia appear normal. Her serum follicle-stimulating hormone, luteinizing hormone, and testosterone are within the reference range. A urine pregnancy test is negative. Which of the following is the most appropriate pharmacotherapy for this patient's condition at this time?
A 23-year-old man is brought to the emergency department by police at 2:00 AM. They picked him up from a local nightclub, where he was yelling and threatening to fight the staff. A review of his medical record is unremarkable. At the hospital, his behavior continues to be agitated and bizarre. His temperature is 37.0°C (98.6°F), the blood pressure is 162/98 mm Hg, the heart rate is 120/min, the respiratory rate is 18/min, and the oxygen saturation is 99% on room air. The physical exam is notable for agitation, but otherwise, he appears healthy. His thin nasal mucosa oozes blood and his pupils are 6mm, equal, and reactive to light. His speech is pressured and bizarre. He insists the hospital should let him go because "I am in the FBI". Urine toxicology is sent to the laboratory for analysis. Which of the following is the most likely cause of this patient's presentation?
A 37-year-old male presents to general medical clinic reporting sleeping difficulties. He states that he has daytime sleepiness, having fallen asleep several times while driving his car recently. He sometimes experiences very vivid dreams just before awakening. You ask the patient's wife if she has witnessed any episodes where her husband lost all muscle tone and fell to the ground, and she confirms that he has not had this symptom. The patient notes that this condition runs in his family, and he desperately asks for treatment. You begin him on a first-line medication for this illness, which works by which mechanism of action?
A 51-year-old man is bitten by a cottonmouth viper and is successfully treated with sheep hyperimmune Fab antivenom. Three days later, the patient develops an abdominal itchy rash and re-presents to the emergency department for medical care. His medical history is significant for gout, hypertension, hypercholesterolemia, diabetes mellitus type II, and multiple basal cell carcinomas on his face and neck. He currently smokes 1 pack of cigarettes per day, drinks a 6-pack of beer per day, and denies any current illicit drug use. His vital signs include: temperature 40.0°C (104.0°F), blood pressure 126/74 mm Hg, heart rate 111/min, and respiratory rate 23/min. On physical examination, his gait is limited by diffuse arthralgias, lung sounds are clear bilaterally, and he has normal heart sounds. The patient has a pruritic periumbilical serpiginous macular rash that has spread to involve the back, upper trunk, and extremities. Of the following options, which is the next best step in patient management?
A 34-year-old woman is recovering in the post-operative unit following a laparoscopic procedure for chronic endometriosis. She had initially presented with complaints of painful menstrual cramps that kept her bedridden most of the day. She also mentioned to her gynecologist that she had been diagnosed with endometriosis 4 years ago, and she could not find a medication or alternative therapeutic measure that helped. Her medical history was significant for surgery she had 6 years ago to remove tumors she had above her kidneys, after which she was prescribed hydrocortisone. An hour after the laparoscopic procedure, she calls the nurse because she is having difficulty breathing. The nurse records her vital signs include: blood pressure 85/55 mm Hg, respirations 20/min, and pulse 115/min. The patient suddenly loses consciousness. Intravenous fluids are started immediately. She gains consciousness, but her blood pressure is unchanged. Which of the following is the most likely cause of the hypotension?
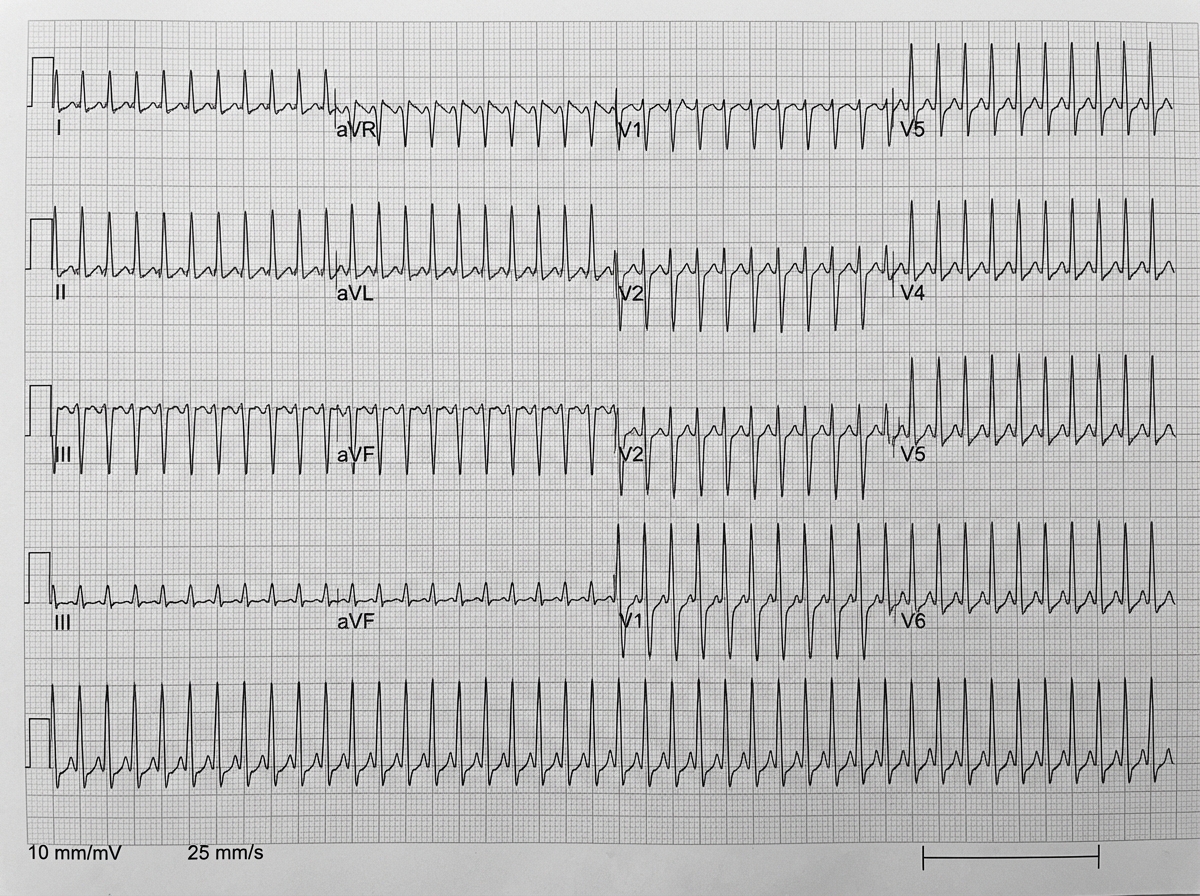
A 26-year-old healthy woman with known heart failure with reduced ejection fraction (HFrEF) presents with lightheadedness, palpitations, and sweating, which started suddenly after she was frightened by her neighbor's dog. The patient's blood pressure is 135/80 mm Hg, the heart rate is 150/min, the respiratory rate is 15/min, and the temperature is 36.6℃ (97.9℉). Her ECG is shown in the exhibit. What is the preferred agent for pharmacologic management of this condition?
A 26-year-old woman comes to the emergency room because she had difficulty breathing during an exercise session. She also has a cough and end-expiratory wheezing. Besides these symptoms, she has a normal physical appearance. She has experienced similar breathing problems during exercise in the past, but never during rest. She is afebrile. What is the best treatment in this case?
Two days after hospitalization for urgent chemotherapy to treat Burkitt’s lymphoma, a 7-year-old boy develops dyspnea and reduced urine output. He also feels a tingling sensation in his fingers and toes. Blood pressure is 100/65 mm Hg, respirations are 28/min, pulse is 100/min, and temperature is 36.2°C (97.2°F). The lungs are clear to auscultation. He has excreted 20 mL of urine in the last 6 hours. Laboratory studies show: Hemoglobin 15 g/dL Leukocyte count 6,000/mm3 with a normal differential serum K+ 6.5 mEq/L Ca+ 7.6 mg/dL Phosphorus 5.4 mg/dL HCO3− 15 mEq/L Uric acid 12 mg/dL Urea nitrogen 44 mg/dL Creatinine 2.4 mg/dL Arterial blood gas analysis on room air: pH 7.30 PCO2 30 mm Hg O2 saturation 95% Which of the following is most likely to have prevented this patient’s condition?
A 21-year-old G1P0 woman presents to the labor and delivery ward at 39 weeks gestation for elective induction of labor. She requests a labor epidural. An epidural catheter is secured at the L4-L5 space. She exhibits no hemodynamic reaction to lidocaine 1.5% with epinephrine 1:200,000. A continuous infusion of bupivacaine 0.0625% is started. After 5 minutes, the nurse informs the anesthesiologist that the patient is hypotensive to 80/50 mmHg with a heart rate increase from 90 bpm to 120 bpm. The patient is asymptomatic and fetal heart rate has not changed significantly from baseline. She says that her legs feel heavy but is still able to move them. What is the most likely cause of the hemodynamic change?
A 25-year-old man presents to the emergency department with a severe pulsatile headache for an hour. He says that he is having palpitations as well. He adds that he has had several episodes of headache in the past which resolved without seeking medical attention. He is a non-smoker and does not drink alcohol. He denies use of any illicit drugs. He looks scared and anxious. His temperature is 37°C (98.6°F), respirations are 25/min, pulse is 107/min, and blood pressure is 221/161 mm Hg. An urgent urinalysis reveals elevated plasma metanephrines. What is the next best step in the management of this patient?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app