
Autonomic/CV Drugs — MCQs

On this page
A research team is studying the effects of a novel drug that was discovered to treat type 2 diabetes. In order to learn more about its effects, they follow patients who are currently taking the drug and determine whether there are adverse effects that exceed anticipated levels and may therefore be drug-related. They discover that the drug causes an excess of sudden cardiac death in 19 patients with renal failure out of 2 million total patients that are followed. Based on these results, an additional warning about this serious adverse effect is added to the investigator brochure for the drug. Which of the following clinical phase studies does this study most likely describe?
A 55-year-old woman comes to the physician because of involuntary hand movements that improve with alcohol consumption. Physical examination shows bilateral hand tremors that worsen when the patient is asked to extend her arms out in front of her. The physician prescribes a medication that is associated with an increased risk of bronchospasms. This drug has which of the following immediate effects on the cardiovascular system? Stroke volume | Heart rate | Peripheral vascular resistance
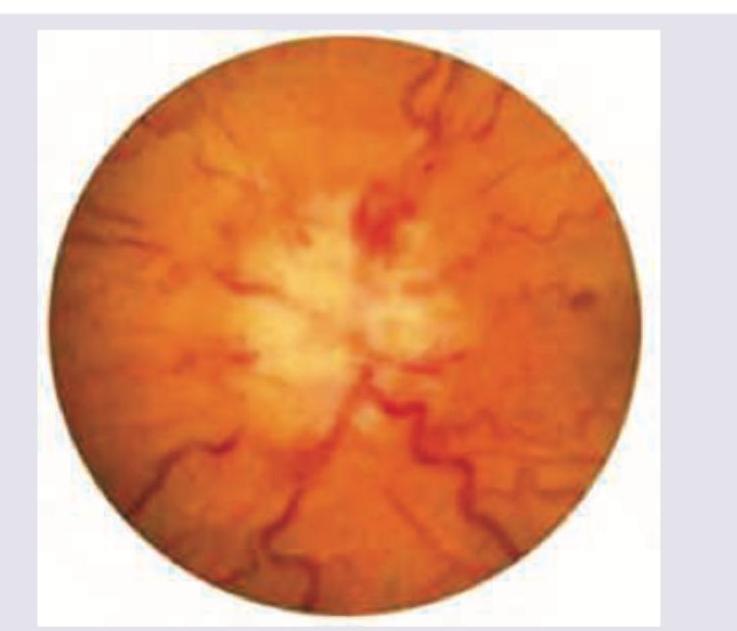
A 30-year-old obese female presents with new-onset headaches, ringing in her ears, and blurry vision. Ibuprofen and avoidance of light has not relieved her symptoms. She denies a history of recent trauma, fever, chills, and fatigue. Past medical history is significant for type 2 diabetes mellitus managed with metformin. She has had 20/20 vision her whole life and wonders if she might need to get eyeglasses. She has 2 healthy school-age children. Her temperature is 36.8°C (98.2°F), heart rate is 90/min, respiratory rate is 15/min, and blood pressure is 135/80 mm Hg. Physical exam is notable for decreased lateral eye movement, and the funduscopic findings are shown in the picture. Laboratory findings are within normal limits and brain imaging is normal. Lumbar puncture demonstrates an elevated opening pressure and normal CSF composition. Which of the following is a side effect of the medication used to treat this condition?
A 66-year-old man with congestive heart failure presents to the emergency department complaining of worsening shortness of breath. These symptoms have worsened over the last 3 days. He has a blood pressure of 126/85 mm Hg and heart rate of 82/min. Physical examination is notable for bibasilar crackles. A chest X-ray reveals bilateral pulmonary edema. His current medications include metoprolol succinate and captopril. You wish to add an additional medication targeted towards his symptoms. Of the following, which statement is correct regarding loop diuretics?
A 26-year-old woman (gravida 3 para 1) with no prenatal care delivers a boy at 37 weeks gestation. His Apgar score is 5 at 1 minute and 8 at 5 minutes. His weight is 2.1 kg (4.2 lb) and length is 47 cm (1 ft 7 in). The mother’s history is significant for chronic pyelonephritis, atrial fibrillation, and gastroesophageal reflux disease. She has a 5-pack-year smoking history and also reports alcohol consumption during pregnancy. Examination of the infant shows a short depressed nasal bridge, wide nose, brachydactyly, and a short neck. Ophthalmoscopy reveals bilateral cataracts. What is the most likely cause of the newborn’s symptoms?
An 8-year-old girl is brought to the physician because of repetitive involuntary movements, including neck twisting, grimacing, grunting, and blinking, for the past 18 months. Her symptoms seem to improve with concentration and worsen with fatigue. During the past 3 months, they have become so severe that she has missed many school days. Her mother says she also has too much anxiety about her involuntary movements to see her friends and prefers staying home in her room. Her birth and development until 18 months ago were normal. Her father suffers from bipolar disorder. Vital signs are within normal limits. Mental status examination shows intact higher mental function and thought processes. Neurological examination shows multiple motor and vocal tics. Physical examination is otherwise within normal limits. Which of the following is the most appropriate initial pharmacotherapy for this condition?
While playing in the woods with friends, a 14-year-old African-American male is bitten by an insect. Minutes later he notices swelling and redness at the site of the insect bite. Which substance has directly led to the wheal formation?
A 34-year-old woman with a history of depression is brought to the emergency department by her husband 45 minutes after ingesting an unknown amount of a termite poison in a suicide attempt. She has abdominal pain, nausea, and vomiting. Her husband reports that she has had two episodes of watery diarrhea on the way to the emergency department. A distinct, garlic-like odor on the breath is noted on examination. An ECG shows sinus tachycardia and QTc prolongation. Administration of which of the following is most appropriate?
A 44-year-old man presents to his primary care physician due to a tremor. His tremor has been progressively worsening over the course of several weeks and he feels embarrassed and anxious about going to social events. He says these movements are involuntary and denies having an urge to have these movements. Medical history is significant for depression which is being treated with escitalopram. His mother is currently alive and healthy but his father committed suicide and had a history of depression. Physical examination is remarkable for impaired saccade initiation and brief, abrupt, and non-stereotyped movements involved the right arm. He also has irregular finger tapping. Which of the following is the best treatment for this patient's symptoms?
A 65-year-old man presents to the emergency department by ambulance following a motor vehicle accident. He was a restrained passenger. At the hospital, he is bleeding heavily from a large wound in his left leg. A review of medical records reveals a history of atrial fibrillation for which he takes warfarin. His international normalized ratio (INR) 2 days ago was 2.6. On physical exam he is cool and clammy. The vital signs include: heart rate 130/min and blood pressure 96/54 mm Hg. Aggressive resuscitation with intravenous normal saline is begun. Which of the following is the next best step to correct this patient's underlying coagulopathy?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app