
Autonomic/CV Drugs — MCQs

On this page
A 25-year-old Caucasian female presents with symptoms of Graves' disease. Her doctor prescribes medications and sends the patient home. After two months of therapy, the patient returns upset that her exophthalmos has not gone away. Which of the following drugs should the physician have prescribed to treat the exophthalmos?
A 23-year-old college student presents with his parents for a follow-up appointment. He was recently diagnosed with schizophrenia and was started on risperidone approx. 2 months ago. He reports a significant improvement since the start of treatment. His parents report that their son’s symptoms of delusions, hallucinations, and paranoid behavior have been ameliorated. On physical examination, the patient seems uncomfortable. He frequently fidgets and repeatedly crosses and uncrosses his legs. When asked if something is troubling him, he gets up and starts pacing. He says, “It’s always like this. I cannot sit still. It is frustrating.” What is the most likely diagnosis?
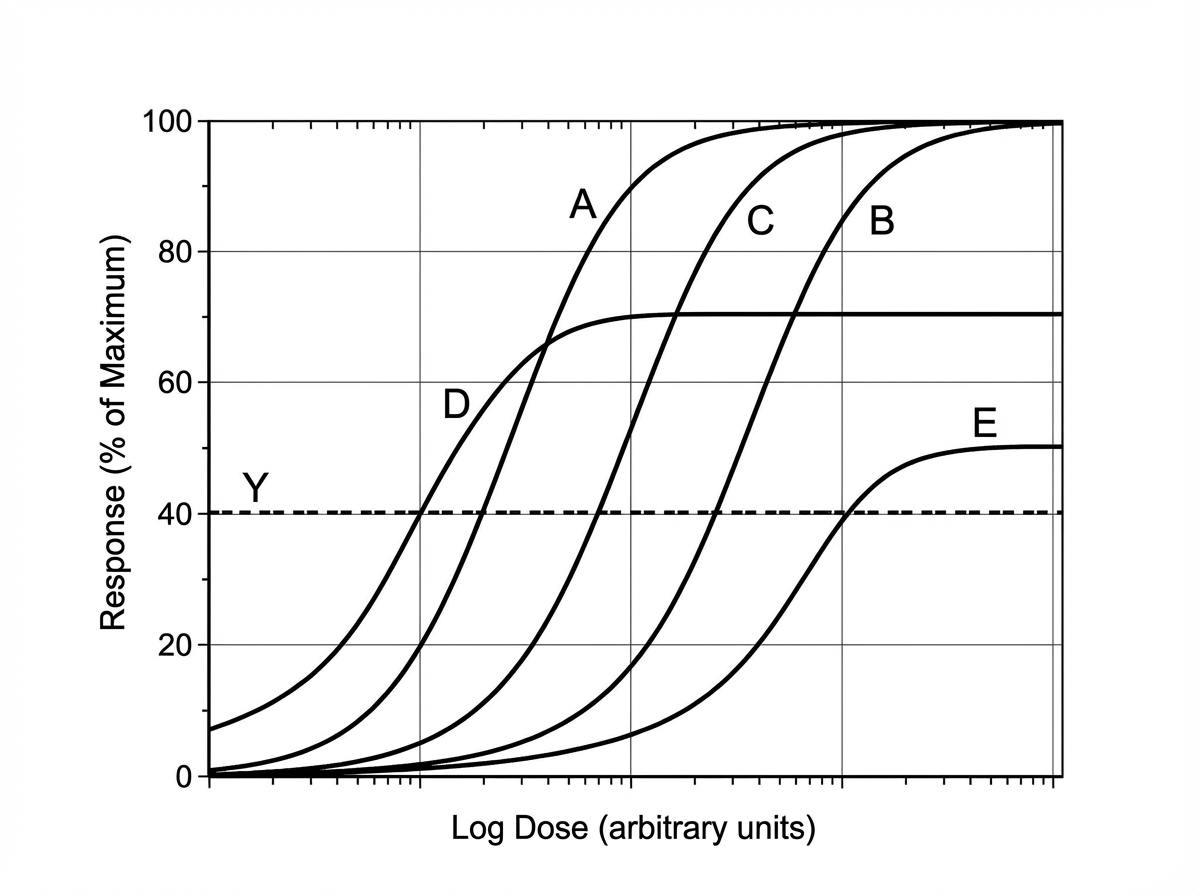
Scientists are developing a new non-steroidal anti-inflammatory drug for osteoarthritis. Their hope is that the new drug will have a higher potency (lower EC50) but the same efficacy as ibuprofen. The scientists also believe that, at the lower doses required due to higher potency, the drug may cause fewer gastrointestinal side effects. If ibuprofen is curve C in the figure provided, which of the following would be the curve for the new drug based on the scientists' specifications? The desired therapeutic effect in patients is represented by the dashed line Y.
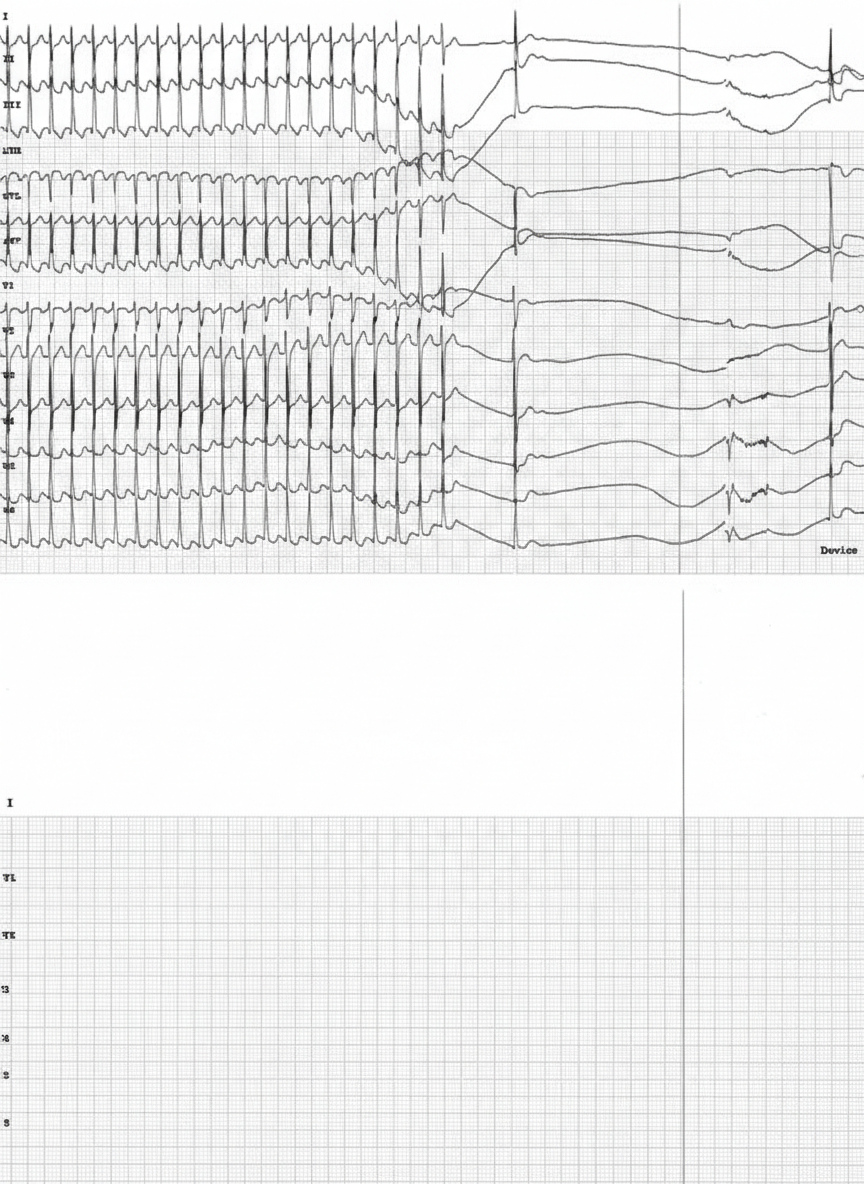
A 46-year-old female is brought to the emergency department by her husband 1 hour after the onset of chest palpitations. Her symptoms began suddenly while she was drinking coffee and have persisted since then. She has not had shortness of breath, chest pain, dizziness, or loss of consciousness. She has experienced these palpitations before, but they typically resolve spontaneously within a few minutes. She has no history of serious illness and takes no medications. Her temperature is 36.8°C (98.2°F), pulse is 155/min, respirations are 18/min, and blood pressure is 130/82 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 97%. Physical examination shows no abnormalities other than tachycardia. An ECG is shown. Repeated, forceful exhalation against a closed glottis while supine fails to relieve her symptoms. Which of the following is the most appropriate next step in management?
A 5-year-old boy is brought to the emergency department by his parents with complaints of severe muscle cramping and abdominal pain. They live in Virginia. The parents state that about 2 hours before, the child was playing in their outdoor shed when he suddenly ran inside crying, saying he was bitten by a bug. One hour following the bite, the child developed the symptoms of cramping and pain. He has no known medical history and takes no medications. His blood pressure is 132/86 mm Hg, the heart rate is 116/min, and the respiratory rate is 20/min. Vital signs reveal tachycardia and hypertension. On exam, there is a 1 cm area of erythema to the dorsum of his right hand without any further dermatologic findings. Palpation of his abdomen reveals firm rigidity but no discernable rebound tenderness. What arthropod is most likely responsible for his symptoms?
A 35-year-old male is picked up by paramedics presenting with respiratory depression, pupillary constriction, and seizures. Within a few minutes, the male dies. On autopsy, fresh tracks marks are seen on both arms. Administration of which of the following medications would have been appropriate for this patient?
An otherwise healthy 49-year-old man presents to his primary care physician for follow-up for a high HbA1C. 3 months ago, his HbA1c was 8.9% on routine screening. Today, after lifestyle modifications, it is 8.1% and his serum glucose is 270 mg/dL. Which of the following is the best initial therapy for this patient's condition?
A 43-year-old woman was admitted to the hospital for anticoagulation following a pulmonary embolism. She was found to have a deep venous thrombosis on further workup after a long plane ride coming back from visiting China. She denies any personal history of blood clots in her past, but she says that her mother has also had to be treated for pulmonary embolism in the recent past. Her past medical history is significant for preeclampsia, hypertension, polycystic ovarian syndrome, and hypercholesterolemia. She currently smokes 1 pack of cigarettes per day, drinks a glass of wine per day, and she currently denies any illicit drug use. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 111/min, and respiratory rate 23/min. On physical examination, her pulses are bounding and complexion is pale, but breath sounds remain clear. Oxygen saturation was initially 81% on room air, with a new oxygen requirement of 8 L by face mask. On day 6 of combined heparin and warfarin anticoagulation, her platelet count decreases from 182,000/mcL to 63,000/mcL. Her international normalized ratio (INR) is not yet therapeutic. What is the next best step in therapy?
A 55-year-old man comes to the physician because of intermittent palpitations that occur when he is stressed, exercising, or when he drinks alcohol. Physical examination shows an irregularly irregular pulse. An ECG shows irregular QRS complexes without any discrete P waves. Pharmacotherapy with carvedilol is initiated for his condition. Compared to treatment with propranolol, which of the following adverse effects is most likely?
A 50-year-old woman is brought to the emergency department following a motor vehicle accident. She is awake but slow to respond. Her breath smells of alcohol. The emergency medical technician reports that her blood pressure has been dropping despite intravenous fluids. Ultrasound reveals a hypoechoic rim around the spleen, suspicious for a splenic laceration. The patient is brought into the operating room for abdominal exploration and a splenic embolization is performed. Since arriving to the hospital, the patient has received 8 units of packed red blood cells and 2 units of fresh frozen plasma. She is stabilized and admitted for observation. The next morning on rounds, the patient complains of numbness and tingling of her mouth and cramping of her hands. Her temperature is 99°F (37.2°C), blood pressure is 110/69 mmHg, and pulse is 93/min. On physical examination, her abdomen is mildly tender without distention. The surgical wound is clean, dry, and intact. Jugular venous pressure is normal. Periodic spasms of the muscles of her bilateral upper and lower extremities can be seen and tapping of the facial nerve elicits twitching of he facial muscles. Which of the following is most likely to improve the patient’s symptoms?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app