
Autonomic/CV Drugs — MCQs

On this page
A 75-year-old man with a 35-pack-year history of smoking is found to be lethargic three days after being admitted with a femur fracture following a motor vehicle accident. His recovery has been progressing well thus far, though pain continued to be present. On exam, the patient is minimally responsive with pinpoint pupils. Vital signs are blood pressure of 115/65 mmHg, HR 80/min, respiratory rate 6/min, and oxygen saturation of 87% on room air. Arterial blood gas (ABG) shows a pH of 7.24 (Normal: 7.35-7.45), PaCO2 of 60mm Hg (normal 35-45mm Hg), a HCO3 of 23 mEq/L (normal 21-28 mEq/L) and a Pa02 of 60 mmHg (normal 80-100 mmHg). Which of the following is the most appropriate therapy at this time?
A 10-year-old boy presents with a painful rash for 1 day. He says that the reddish, purple rash started on his forearm but has now spread to his abdomen. He says there is a burning pain in the area where the rash is located. He also says he has had a stuffy nose for several days. Past medical history is significant for asthma and epilepsy, medically managed. Current medications are a daily chewable multivitamin, albuterol, budesonide, and lamotrigine, which was initiated several weeks ago. On physical examination, there is a red-purple maculopapular rash present on upper extremities and torso. There are some blisters present over the rash, as shown in the image, which is also present in the oral mucosa. Which of the following is the most likely cause of this patient's symptoms?

A 64-year-old man is brought to the emergency department because of dull lower abdominal pain for 3 hours. He has not urinated for 24 hours and has not passed stool for over 3 days. He was diagnosed with herpes zoster 4 weeks ago and continues to have pain even after his rash resolved. He has hypertension, benign prostatic hyperplasia, and coronary artery disease. Physical examination shows a tender, palpable suprapubic mass. Bowel sounds are hypoactive. Abdominal ultrasound shows a large anechoic mass in the pelvis. Which of the following drugs most likely accounts for this patient's current symptoms?
A 16-year-old girl who recently immigrated to the United States from Bolivia presents to her primary care physician with a chief complaint of inattentiveness in school. The patient's teacher describes her as occasionally "day-dreaming" for periods of time during which the patient does not respond or participate in school activities. Nothing has helped the patient change her behavior, including parent-teacher conferences or punishment. The patient has no other complaints herself. The only other concern that the patient's mother has is that upon awakening she notices that sometimes the patient's arm will jerk back and forth. The patient states she is not doing this intentionally. The patient has an unknown past medical history and is currently not on any medications. On physical exam you note a young, healthy girl whose neurological exam is within normal limits. Which of the following is the best initial treatment?
An experimental new drug (SD27C) is being studied. This novel drug delivers insulin via the intranasal route. Consent is obtained from participants who are diabetic and are taking insulin as their current treatment regimen to participate in a clinical trial. 500 patients consent and are divided into 2 groups, and a double-blind clinical trial was conducted. One group received the new formulation (SD27C), while the second group received regular insulin via subcutaneous injection. The results showed that the treatment outcomes in both groups are the same. SD27C is currently under investigation in which phase of the clinical trial?
A 52-year-old woman presents to her primary care provider with shortness of breath. She reports a 3-month history of difficulty breathing with exertion that has progressed to affect her at rest. She swims 45 minutes every day but has had trouble swimming recently due to her breathing difficulties. Her past medical history is notable for well-controlled mild intermittent asthma and generalized anxiety disorder. She has a 15 pack-year smoking history but quit 15 years ago. She does not drink alcohol. Her mother died at the age of 60 from heart failure and was a lifetime non-smoker. Her temperature is 99°F (37.2°C), blood pressure is 135/85 mmHg, pulse is 85/min, and respirations are 22/min. Her BMI is 23 kg/m^2. On exam, she has slightly increased work of breathing. Cardiac auscultation reveals a normal S1 and loud P2. An echocardiogram is performed demonstrating right ventricular hypertrophy. Her pulmonary artery pressure is 24 mmHg at rest and 40 mmHg with exercise. This patient’s condition is associated with a mutation in a gene that does which of the following?
A 58-year-old woman presents to the physician for a routine health maintenance examination. She has a history of dyslipidemia and chronic hypertension. Her medications include atorvastatin, hydrochlorothiazide, and lisinopril. She exercises every day and follows a healthy diet. She does not smoke. There is no family history of chronic disease. Her blood pressure is 130/80 mm Hg, which is confirmed on repeat measurement. Her BMI is 22 kg/m2. The physical examination shows no abnormal findings. The laboratory test results show: Serum Total cholesterol 193 mg/dL Low-density lipoprotein (LDL-C) 124 mg/dL High-density lipoprotein (HDL-C) 40 mg/dL Triglycerides 148 mg/dL The patient's 10-year risk of cardiovascular disease (CVD) is 4.6%. Which of the following is the most appropriate next step in pharmacotherapy?
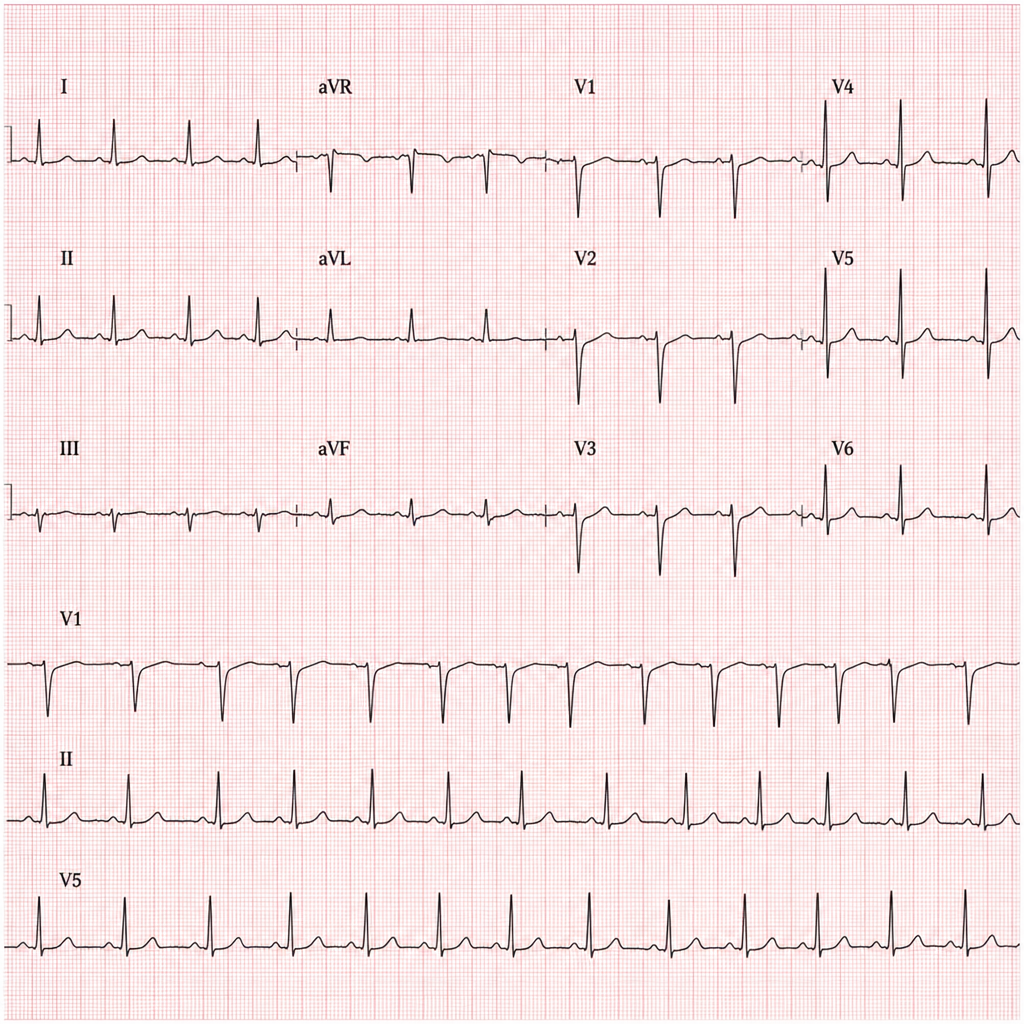
An 18-year-old high school student is brought to the emergency department after collapsing during her cheerleading practice session. She was brought to the hospital even though she regained consciousness within seconds. Her mother informs the doctor that she had a similar episode last month at a party, but they thought it was due to stress and exhaustion. Both incidents occurred in a loud and crowded environment. Her past medical history is insignificant. Her blood pressure is 120/80 mm Hg and the pulse is 77/min and regular. Physical examination findings are within normal limits. A set of tests are ordered along with a 12-lead ECG. The ECG tracing obtained is shown. What is the best treatment option for this patient?
A 58-year-old man comes to the physician because of severe muscle aches and fatigue for 3 days. Last week he was diagnosed with atypical pneumonia and treated with clarithromycin. He has hyperlipidemia for which he takes lovastatin. Physical examination shows generalized tenderness of the proximal muscles in the upper and lower extremities. Serum studies show an elevated creatine kinase concentration. This patient's current symptoms are most likely caused by inhibition of which of the following hepatic enzymes?
A 66-year-old male with a history of deep venous thrombosis is admitted to the hospital with shortness of breath and pleuritic chest pain. He is treated with an anticoagulant, but he develops significant hematochezia. His BP is now 105/60 and HR is 117; both were within normal limits on admission. The effects of the anticoagulant are virtually completely reversed with the administration of protamine. Which of the following was the anticoagulant most likely administered to this patient?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app