
Autonomic/CV Drugs — MCQs

On this page
A 67-year-old man presents to his primary care physician for a decline in his hearing that he noticed over the past week. The patient has a past medical history of hypertension and diabetes mellitus and was recently diagnosed with bladder cancer which is currently appropriately being treated. The patient is a hunter and often goes shooting in his spare time. His recent sick contacts include his grandson who is being treated with amoxicillin for ear pain. Physical exam is notable for decreased hearing bilaterally. The Weber test does not localize to either ear, and the Rinne test demonstrates air conduction is louder than bone conduction. Which of the following is the most likely etiology for this patient's hearing loss?
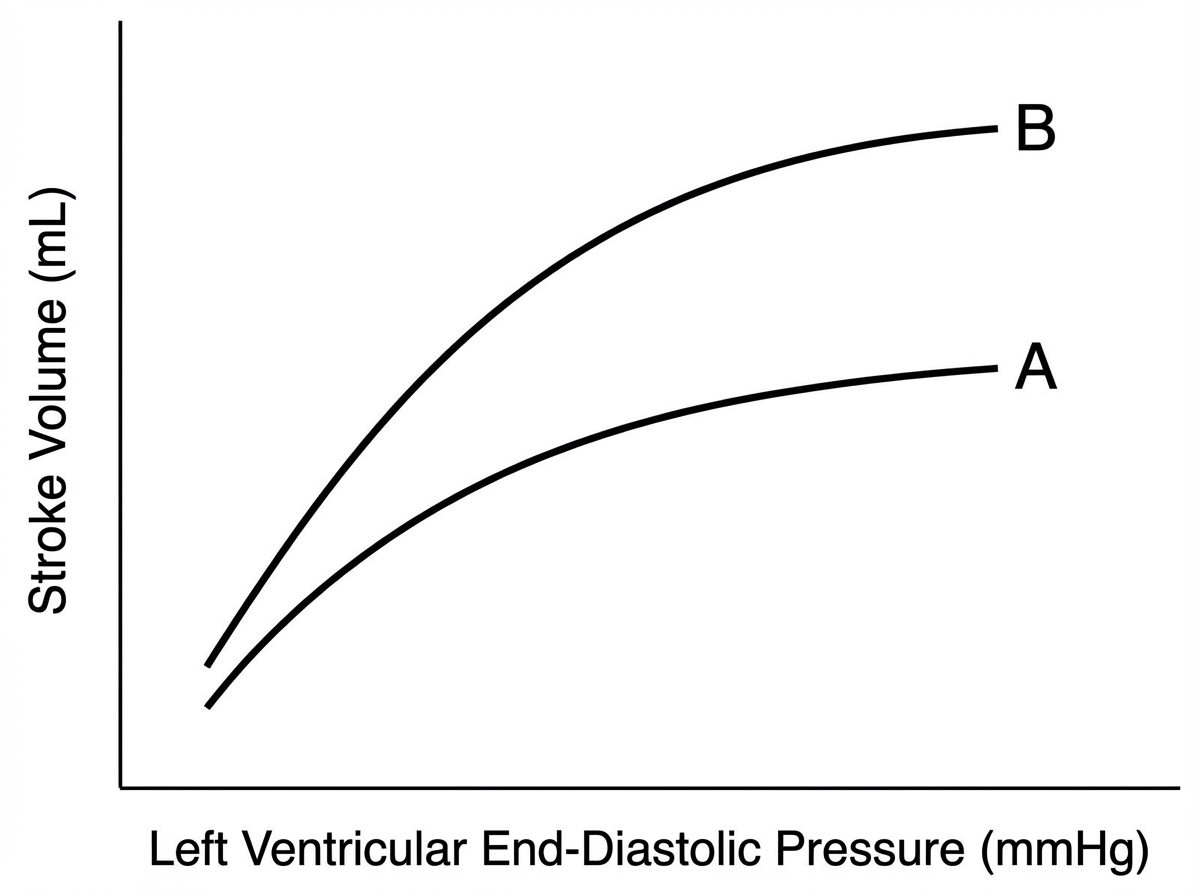
A 78-year-old male comes to the physician’s office for a routine check-up. He complains of increased lower extremity swelling, inability to climb the one flight of stairs in his home, and waking up in the middle of the night 2-3 times gasping for breath. He has had to increase the number of pillows on which he sleeps at night. These symptoms started 9 months ago and have been progressing. The doctor starts him on a medication regimen, one of which changes his Starling curve from A to B as shown in the Figure. Which of the following medications is most consistent with this mechanism of action?
Benzodiazepines are clinically useful because of their inhibitory effects on the central nervous system. Which of the following correctly pairs the site of action of benzodiazepines with the molecular mechanism by which they exert their effects?
A 45-year-old man with type 2 diabetes mellitus presents to his family physician for a follow-up appointment. He is currently using a 3-drug regimen consisting of metformin, sitagliptin, and glipizide. Despite this therapeutic regimen, his most recent hemoglobin A1c level is 8.1%. Which of the following is the next best step for this patient?
A 37-year-old woman presents to the emergency department with a chief complaint of severe pain in her face. She states that over the past week she has experienced episodic and intense pain in her face that comes on suddenly and resolves on its own. She states she feels the pain over her cheek and near her eye. The pain is so severe it causes her eyes to tear up, and she is very self conscious about the episodes. She fears going out in public as a result and sometimes feels her symptoms come on when she thinks about an episode occurring while in public. While she is waiting in the emergency room her symptoms resolve. The patient has a past medical history of diabetes, constipation, irritable bowel syndrome, and anxiety. She is well known to the emergency department for coming in with chief complaints that often do not have an organic etiology. Her temperature is 99.5°F (37.5°C), blood pressure is 177/108 mmHg, pulse is 90/min, respirations are 17/min, and oxygen saturation is 98% on room air. Cardiopulmonary and abdominal exams are within normal limits. Neurological exam reveals cranial nerves II-XII are grossly intact. The patient's pupils are equal and reactive to light. Pain is not elicited with palpation of the patient's face. Which of the following is the best initial step in management?
A 14-year-old boy presents to an urgent care clinic complaining of a runny nose that has lasted for a few weeks. He also reports sneezing attacks that last up to an hour, nasal obstruction, and generalized itching. He has similar episodes each year during the springtime that prevent him from going out with his friends or trying out for sports. His younger brother has a history of asthma. Which of the following diseases has a similar pathophysiology?
A 60-year-old woman presents to the emergency department with progressive nausea and vomiting. She reports that approximately one day prior to presentation she experienced abdominal discomfort that subsequently worsened to severe nausea, vomiting, and two episodes of watery diarrhea. She recently noticed that her vision has become blurry along with mild alterations in color perception. Medical history is significant for congestive heart failure with a low ejection fraction. She cannot recall which medications she is currently taking but believes she is taking them as prescribed. Which of the following is a characteristic of the likely offending drug that led to this patient’s clinical presentation?
A 24-year-old obese woman presents with a severe right-sided frontotemporal headache that started 2 days ago. There is no improvement with over-the-counter pain medications. Yesterday, the pain was so intense that she stayed in bed all day in a dark, quiet room instead of going to work. This morning she decided to come in after an episode of vomiting. She says she has experienced 5–6 similar types of headaches each lasting 12–24 hours over the last 6 months but never this severe. She denies any seizures, visual disturbances, meningismus, sick contacts or focal neurologic deficits. Her past medical history is significant for moderate persistent asthma, which is managed with ipratropium bromide and an albuterol inhaler. She is currently sexually active with 2 men, uses condoms consistently, and regularly takes estrogen-containing oral contraceptive pills (OCPs). Her vital signs include: blood pressure 122/84 mm Hg, pulse 86/min, respiratory rate 19/min, and blood oxygen saturation (SpO2) 98% on room air. Physical examination, including a complete neurologic exam, is unremarkable. A magnetic resonance image (MRI) of the brain appears normal. Which of the following is the best prophylactic treatment for this patient’s most likely condition?
A 55-year-old man comes to the physician for a follow-up examination. He feels well. He has hyperlipidemia and type 2 diabetes mellitus. He takes medium-dose simvastatin and metformin. Four months ago, fasting serum studies showed a LDL-cholesterol of 136 mg/dL and his medications were adjusted. Vital signs are within normal limits. On physical examination, there is generalized weakness of the proximal muscles. Deep tendon reflexes are 2+ bilaterally. Fasting serum studies show: Total cholesterol 154 mg/dL HDL-cholesterol 35 mg/dL LDL-cholesterol 63 mg/dL Triglycerides 138 mg/dL Glucose 98 mg/dL Creatinine 1.1 mg/dL Creatine kinase 260 mg/dL Which of the following is the most appropriate next step in management of this patient's hyperlipidemia?
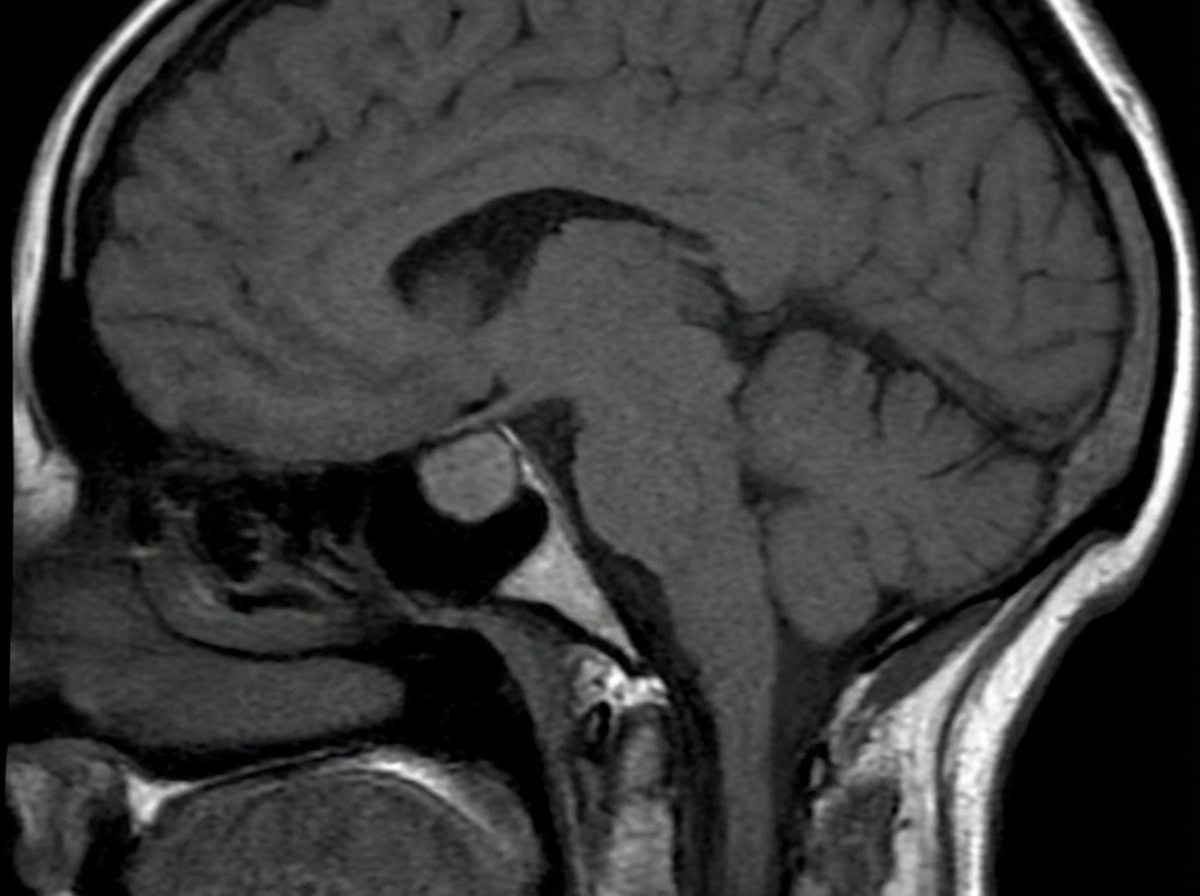
A 35-year-old woman comes to the physician because of headaches, irregular menses, and nipple discharge for the past 4 months. Breast examination shows milky white discharge from both nipples. Her thyroid function tests and morning cortisol concentrations are within the reference ranges. A urine pregnancy test is negative. An MRI of the brain is shown. Which of the following sets of changes is most likely in this patient? $$$ Serum estrogen %%% Serum progesterone %%% Dopamine synthesis $$$
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app