
Autonomic/CV Drugs — MCQs

On this page
A 53-year-old woman presents for a follow-up. She took some blood tests recently for her yearly physical, and her random blood sugar level was found to be 251 mg/dL. She was asked to repeat her blood sugar and come back with the new reports. At that time, her fasting blood sugar level was 130 mg/dL and the postprandial glucose level was 245 mg/dL. Her HbA1c is 8.9%. She has had occasions where she felt light-headed and felt better only after she had something to eat. Her physician starts her on a drug to help her control her sugar levels. He also advised that she should return for routine follow-up labs and repeat HbA1c in 3 months. Which of the following is the mechanism of action of the drug that she was most likely prescribed?
A 58-year-old woman presents to her primary care physician for a wellness checkup. She recently had a DEXA scan that placed her at 2 standard deviations below the mean for bone density. She is following up today to discuss her results. The patient has a past medical history of asthma, breast cancer, COPD, anxiety, irritable bowel syndrome, endometrial cancer, and depression. She is currently taking clonazepam, albuterol, and fluoxetine. Her temperature is 99.5°F (37.5°C), blood pressure is 127/68 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 95% on room air. The patient is treated appropriately and sent home. She returns 1 month later for a follow up visit. She has been taking her medications as prescribed. She endorses episodes of feeling febrile/warm which resolve shortly thereafter. Otherwise she is doing well. Which of the following is true of the medication she was most likely started on?
A 10-year-old girl is brought to the neurologist for management of recently diagnosed seizures. Based on her clinical presentation, the neurologist decides to start a medication that works by blocking thalamic T-type calcium channels. Her parents are cautioned that the medication has a number of side effects including itching, headache, and GI distress. Specifically, they are warned to stop the medication immediately and seek medical attention if they notice skin bullae or sloughing. Which of the following conditions is most likely being treated in this patient?
A 42-year-old female with a history of systemic lupus erythematosus (SLE) has a 3-year history of daily prednisone (20 mg) use. Due to long-term prednisone use, she is at increased risk for which of the following?
An 8-year-old female is given omalizumab for the treatment of bronchial asthma. Omalizumab treats asthma through which mechanism?
A 49-year-old man seeks evaluation at an urgent care clinic with a complaint of palpitations for the past few hours. He denies any chest pain, shortness of breath, or sweating. He is anxious and appears worried. His medical history is unremarkable with the exception of mild bronchial asthma. He only uses medications during an asthma attack and has not used medications since last week. He is a former smoker and drinks a couple of beers on weekends. His heart rate is 146/min, respiratory rate is 16/min, temperature is 37.6°C (99.68°F), and blood pressure is 120/80 mm Hg. The physical examination is unremarkable, and an electrocardiogram is ordered. Which of the following groups of drugs should be given to treat his symptoms?
A 62-year-old man is brought to the emergency room because of pain in his right hip. He was found lying on the floor several hours after falling onto his right side. Ten years ago, he received a renal transplant from a living related donor. He has a 4-year history of type 2 diabetes. Current medications include prednisone, cyclosporine, and metformin. Examination shows a shortened and externally rotated right leg. There is extensive bruising over the right buttock and thigh. X-ray of the right hip shows a displaced femoral neck fracture. The patient is resuscitated in the emergency room and taken to surgery for a right total hip replacement. Post-operative laboratory studies show: Hemoglobin 11.2 g/dL Serum Na+ 148 mmol/L K+ 7.1 mmol/L Cl- 119 mmol/L HCO3- 18 mmol/L Urea nitrogen 22 mg/dL Creatinine 1.6 mg/dL Glucose 200 mg/dL Creatine kinase 1,562 U/L His urine appears brown. Urine dipstick is strongly positive for blood. ECG shows peaked T waves. Intravenous calcium gluconate is administered. What is the most appropriate next step in management?
A 65-year-old woman, with end-stage renal disease (ESRD) on hemodialysis, presents with pain, swelling and discoloration of her right leg and foot. She says that she started twice-weekly hemodialysis 2 weeks ago and has had no issues until 1 week ago when she noticed a warm, painful swelling of the back of her right leg and right foot after finishing her dialysis session. Over the week, she says these symptoms have steadily worsened and, in the last few days, her right foot has become discolored. Past medical history is significant for ESRD secondary to long-standing hypertension. Current medications are verapamil 200 mg orally daily and unfractionated heparin that is given during hemodialysis. Her vital signs include: temperature 37.0°C (98.6°F), blood pressure 145/75 mm Hg, pulse 88/min, respirations 15/min, and oxygen saturation 99% on room air. On physical examination, the patient is alert and cooperative. The cardiac exam is normal. Lungs are clear to auscultation. The abdomen is soft and nontender with no hepatosplenomegaly. The right calf is swollen, warm, and erythematous. Physical findings of the patient’s right foot are shown in the exhibit. Laboratory findings are significant for the following: Sodium 141 mEq/L Potassium 4.9 mEq/L Chloride 104 mEq/L Bicarbonate 25 mEq/L BUN 32 mg/dL Creatinine 3.1 mg/dL Glucose (fasting) 75 mg/dL Bilirubin, conjugated 0.5 mg/dL Bilirubin, total 1.0 mg/dL AST (SGOT) 22 U/L ALT (SGPT) 23 U/L Alkaline phosphatase 56 U/L Bleeding time 19 min Prothrombin time (PT) 11 s Partial thromboplastin time (PTT) 30 s WBC 8,500/mm3 RBC 4.10 x 106/mm3 Hematocrit 41.5% Hemoglobin 13.5 g/dL Platelet count 100,000/mm3 (previously 200,000/mm3) Which of the following is the next best diagnostic step in this patient?

A 58-year-old Caucasian male who is being treated for atrial fibrillation and angina complains of dyspnea on exertion. On exam, his heart rate 104-115/min and irregularly irregular at rest. He has no chest pain. You believe his rate control for atrial fibrillation is suboptimal and the likely cause of his dyspnea. You are considering adding verapamil to his current metoprolol for additional rate control of his atrial fibrillation. Which of the following side effects should you be most concerned about with this additional medication?
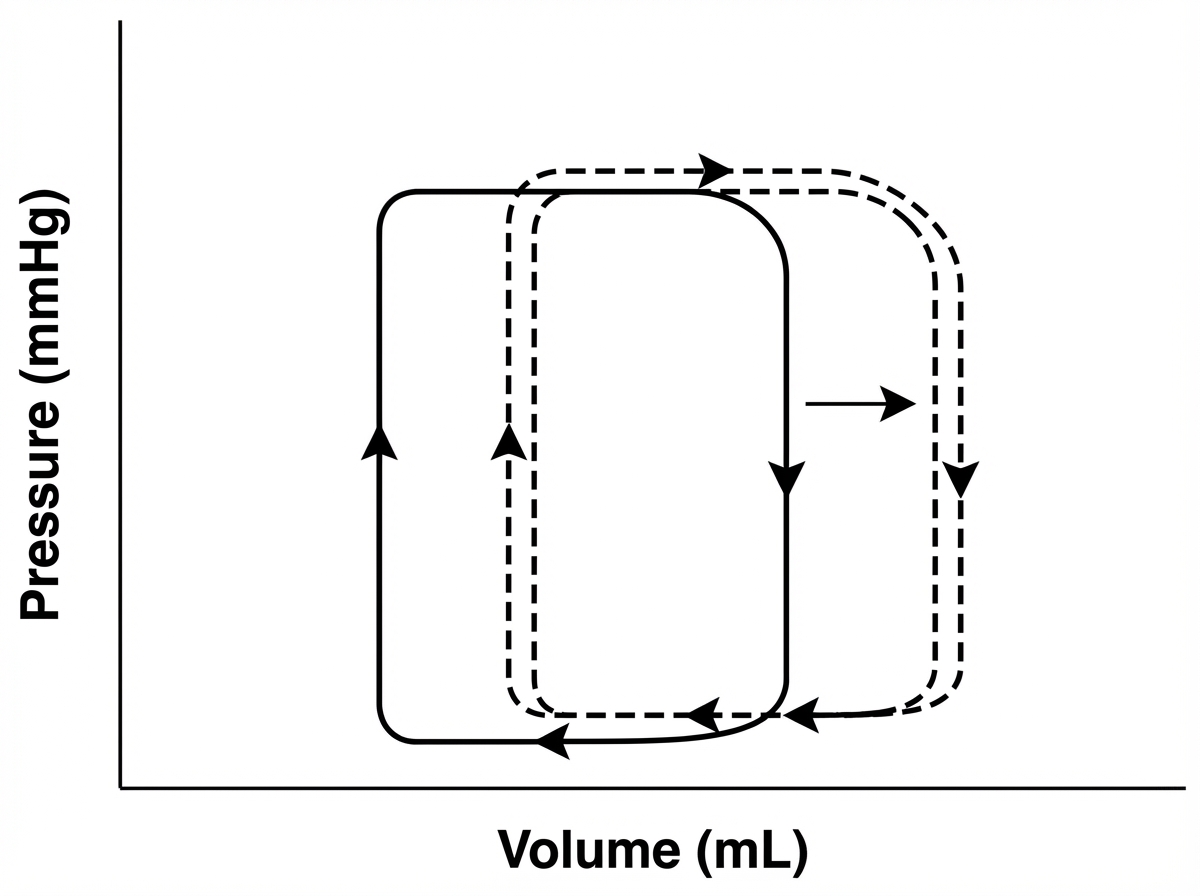
A pharmaceutical company is testing a new antidepressant. During phase I of the drug trial, healthy volunteers are recruited, and the effects of the drug on the cardiovascular system are studied. A graphical representation of the volume-pressure relationship of the left ventricle of the heart is given below with the dashed line representing post medication changes. Which of the following is the most likely mechanism of the drug being studied?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app