
Autonomic/CV Drugs — MCQs

On this page
A 21-year-old woman with type 1 diabetes mellitus suddenly develops tremors, cold sweats, and confusion while on a backpacking trip with friends. She is only oriented to person and is unable to follow commands. Her fingerstick blood glucose concentration is 28 mg/dL. Her friend administers an intramuscular injection with a substance that reverses her symptoms. Which of the following is the most likely mechanism of action of this drug?
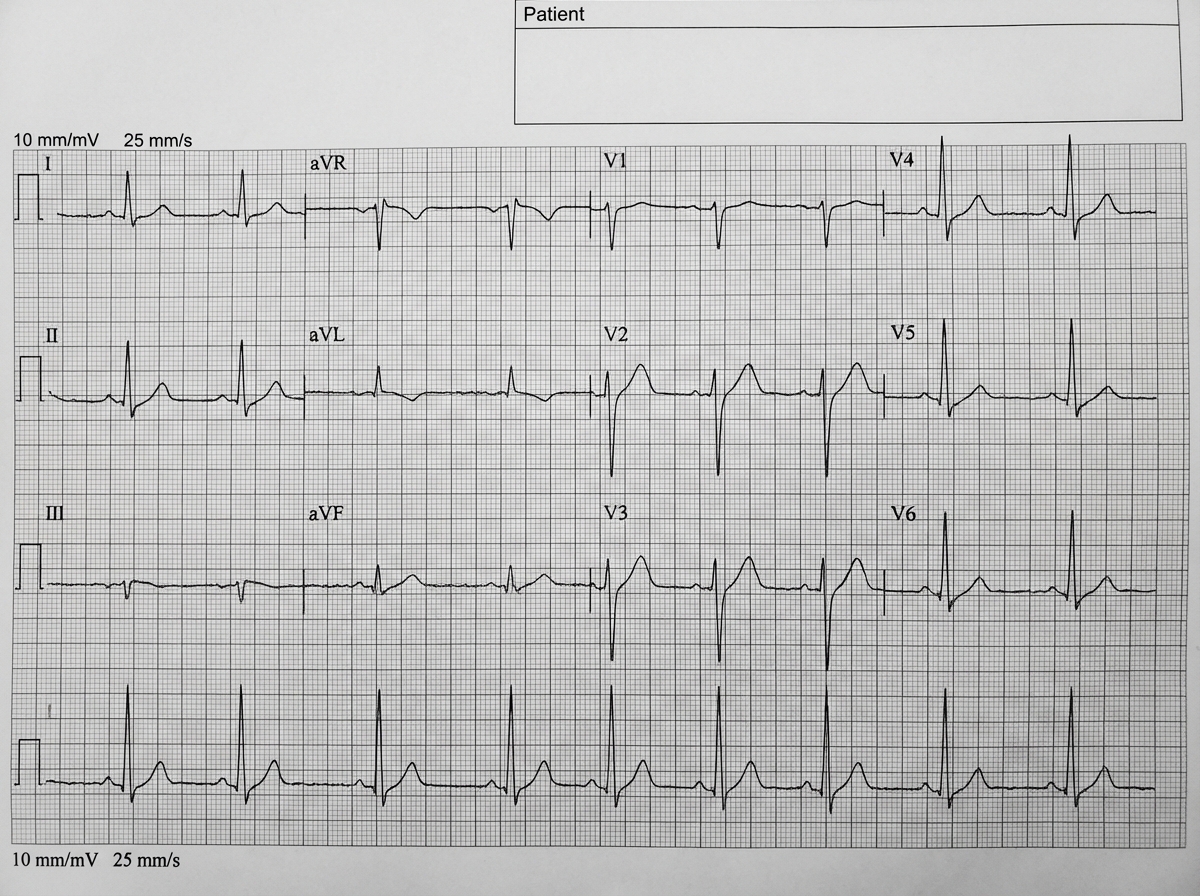
A 17-year-old boy was brought to the emergency department because of palpitations and lightheadedness that began 16 hours ago. He admitted to binge drinking the night before. He was sedated and electrically cardioverted. An ECG that was recorded following cardioversion is shown, demonstrating a shortened PR interval, delta waves, and widened QRS complexes consistent with Wolff-Parkinson-White (WPW) syndrome. After regaining consciousness, he was admitted for observation. Serum concentration of creatinine and electrolytes were measured to be within the reference range. Twelve hours after cardioversion, the patient complains again of palpitations. He does not have lightheadedness or chest pain. His temperature is 37.1°C (98.8°F), pulse is 220/min, respirations are 20/min, and blood pressure is 112/84 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 98%. Physical examination shows no abnormalities. A newly recorded ECG shows wide QRS complexes with an irregular rhythm and variable QRS morphology. Which of the following is the most appropriate next best step in management?
A 49-year-old man with alcohol use disorder is brought to the emergency department immediately after two episodes of coffee-ground emesis. His pulse is 116/min and blood pressure is 92/54 mm Hg. Physical examination shows a distended abdomen with shifting dullness. Skin examination shows jaundice, erythematous palms, and dilated veins in the anterior abdominal wall. After fluid resuscitation, he is given a drug that decreases portal venous pressure. The drug works by inhibiting the secretion of splanchnic vasodilatory hormones as well as blocking glucagon and insulin release. This drug is a synthetic analog of a substance normally produced in which of the following cells?
A 24-year-old man presents to his family practitioner for routine follow-up of asthma. He is currently on albuterol, corticosteroids, and salmeterol, all via inhalation. The patient is compliant with his medications, but he still complains of episodic shortness of breath and wheezing. The peak expiratory flow (PEF) has improved since the last visit, but it is still less than the ideal predicted values based on age, gender, and height. Montelukast is added to his treatment regimen. What is the mechanism of action of this drug?
A 24-year-old woman, gravida 2, para 1, at 33 weeks’ gestation, is admitted to the hospital for treatment of preterm labor. She has no history of serious illness and her only medication is a multivitamin. Her temperature is 37.2°C (99.0°F), pulse is 100/min, respirations are 20/min, and blood pressure is 100/75 mm Hg. Therapy with nifedipine and betamethasone is begun. The patient continues to have contractions; nifedipine is discontinued and treatment with high-dose terbutaline is initiated. Her contractions resolve. Three hours later, the patient reports fatigue and weakness. Neurologic examination shows proximal muscle weakness of the lower extremities. Deep tendon reflexes are 1+ bilaterally. Which of the following is most likely to confirm the diagnosis?
A 48-year-old male with a history of rhinitis presents to the emergency department with complaints of shortness of breath and wheezing over the past 2 days. He reports bilateral knee pain over the past month for which he recently began taking naproxen 1 week ago. Physical examination is significant for a nasal polyp and disappearance of bilateral radial pulses on deep inspiration. Which of the following is the most likely cause of this patient's physical examination findings?
A 58-year-old female presents to her primary care physician with a 1-month history of facial and chest flushing, as well as intermittent diarrhea and occasional difficulty breathing. On physical exam, a new-onset systolic ejection murmur is auscultated and is loudest at the left second intercostal space. Subsequent echocardiography reveals leaflet thickening secondary to fibrous plaque deposition on both the pulmonic and tricuspid valves. Which of the following laboratory abnormalities would most likely be found in this patient?
One month after undergoing surgical spinal fusion because of a traumatic spinal cord injury, a 68-year-old man comes to the physician because of lower abdominal pain. He last voided yesterday. Physical examination shows a suprapubic mass and decreased sensation below the umbilicus. Urodynamic studies show simultaneous contractions of the detrusor muscle and the internal urethral sphincter. Urinary catheterization drains 900 mL of urine from the bladder. Which of the following is the most appropriate pharmacotherapy for this patient’s urinary symptoms?
A 24-year-old African American male with sickle cell disease has been followed by a hematologist since infancy. Two years ago, he was started on hydroxyurea for frequent pain crises but has not achieved good control. The addition of a Gardos channel blocking agent is being considered. What is the mechanism of action of this class of medications?
A 60-year-old woman presents to you with vision problems. Objects appear clear, but she just can't see as well as before. She says she first noticed this when she went to the movies with her grandkids, and she could not see the whole screen. She denies any complaints of redness, itchiness, or excessive tearing of her eyes. Current medications are captopril for her hypertension, acetaminophen for occasional headaches, and a daily multivitamin. Her vital signs are a blood pressure 130/80 mm Hg, pulse 80/min and regular, respiratory rate 14/min, and a temperature of 36.7°C (98.0°F). Eye examination reveals that her visual acuity is normal but the visual field is reduced with enlarged blind spots. Tonometry reveals mildly increased IOP. The patient is started on brimonidine. Which of the following statements best describes the therapeutic mechanism of action of this medication in this patient?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app