
Autonomic/CV Drugs — MCQs

On this page
A 49-year-old man comes to the physician because of a 5-month history of progressive fatigue and exertional dyspnea. Cardiac examination shows a loud S2 in the 2nd left intercostal space. Right heart catheterization shows a pulmonary artery pressure of 32 mm Hg. Treatment with bosentan is initiated. The beneficial effect of this drug is due to binding to which of the following?
A 69-year-old woman with type 2 diabetes mellitus has an HbA1c of 7.9% and has been using basal-bolus insulin to manage her diabetes for the past 5 years. She has been maintaining a healthy diet, taking her insulin as scheduled but her records show morning hyperglycemia before eating breakfast. To determine the cause of this hyperglycemia, you ask her to set an alarm and take her blood glucose at 3 am. At 3 am her blood glucose is 49 mg/dL. Which of the following statements best describes the management of this patient's current condition?
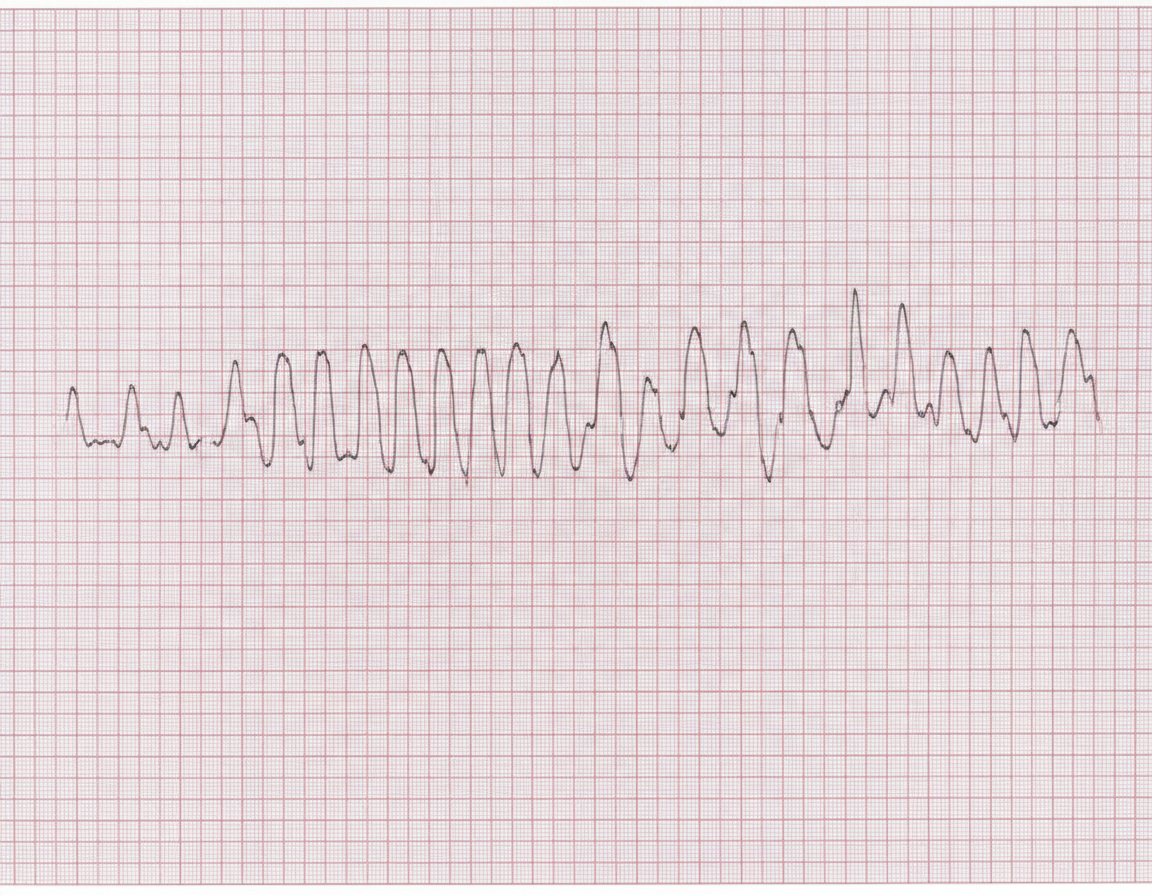
A 44-year-old woman is admitted after an episode of dizziness and palpitations with a subsequent loss of consciousness. At the time of admission, the patient is alert, but then quickly becomes lethargic and reports reoccurrence of palpitations. Past medical history is significant for an episode of ventricular tachycardia 4 months ago, now managed with pharmacologic antiarrhythmic prophylaxis. An ECG is obtained and is shown on the image. Which of the following antiarrhythmic drugs is most likely responsible for this patient's condition?
A 48-year-old homeless man is brought to the emergency department 2 hours after his right arm was burned by a fire. He is diagnosed with extensive third-degree burns of the right forearm and upper arm and is admitted to the hospital for debridement and grafting. During his stay in the hospital, he suddenly develops confusion and agitation. Neurologic examination shows horizontal nystagmus and a broad-based gait. Laboratory studies show decreased erythrocyte transketolase activity. Administration of which of the following most likely caused this patient's current condition?
A 7-year-old boy is brought to the physician by his mother because of a 2-week history of intermittent shortness of breath and a dry cough that is worse at night. He had an upper respiratory tract infection 3 weeks ago. Lungs are clear to auscultation. Spirometry shows normal forced vital capacity and peak expiratory flow rate. The physician administers a drug, after which repeat spirometry shows a reduced peak expiratory flow rate. Which of the following drugs was most likely administered?
A 27-year-old woman presents to the clinic with a runny nose and productive cough for the past two weeks. She also complains of headaches and lethargy. She was started on sertraline after she was diagnosed with major depressive disorder 2 months ago and had the dosage periodically increased to achieve symptom control. She is afraid of starting any other medication because of possible side-effects or life-threatening drug interactions. What advice is most accurate regarding possible complications to her current pharmacotherapy?
A 28-year-old woman presents with severe diarrhea and abdominal pain. She says she has had 10 watery stools since the previous morning and is experiencing severe cramping in her abdomen. She reports similar past episodes of diarrhea with excruciating abdominal pain and mentions that she has taken diphenoxylate and atropine before which had helped her diarrhea and pain but resulted in severe constipation for a week. Which of the following receptors does diphenoxylate activate to cause the effects mentioned by this patient?
A 28-year-old man presents to his primary care physician because he has been experiencing constipation for the last 6 days. He says that the constipation started 1 day after he started taking an over the counter medication for sinus congestion and a chronic cough. He has no other findings associated with the constipation. His past medical history is significant for seasonal allergies but he is not currently taking any other medications besides the one he reported. Which of the following drugs was most likely responsible for this patient's symptoms?
A 30-year-old man presents with a 1-month history of frequent intermittent headaches. He says the headaches typically occur between 3–4 times/day, mostly at night, each lasting minutes to 1–2 hours. He describes the pain as severe, stabbing, unilateral, and localized to the left periorbital region. He says he frequently notes increased tear production and conjunctival injection in the left eye and rhinorrhea during these headaches. He mentions that he had a similar 3-week episode of these same, frequent intermittent headaches 3 months ago which stopped completely until 1 month ago. He denies any seizures, loss of consciousness, nausea, vomiting, photophobia, or phonophobia. His past medical history is significant for stable angina secondary to coronary artery disease diagnosed on a stress echocardiogram 1 year ago. He reports occasional alcohol use, which he says precipitates the headaches, but denies any smoking or recreational drug use. The patient is afebrile, and his vital signs are within normal limits. A physical examination is unremarkable. A noncontrast computed tomography (CT) scan of the head is normal. Which of the following is the best abortive treatment for this patient?
A 55-year-old obese woman is referred to the cardiology clinic for progressive dyspnea. She has had no recent travel or sick contacts. Besides a multivitamin, she has only tried online weight-loss medications for the past five years, including fenfluramine-phentermine. An echocardiogram reveals a dilated right ventricle with systolic pressure of 60 mmHg as well as both tricuspid and pulmonary regurgitation. A right heart catheterization shows a mean pulmonary artery pressure of 40 mmHg. What disease process is most analogous to this patient's presentation?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app