
Autonomic/CV Drugs — MCQs

On this page
A goalkeeper of a famous soccer team gives an interview with a health agency regarding his childhood. He describes how when he was a child, he would constantly clear his throat in class and the teachers would write a note to his mother with advice to go see an ENT doctor. He complained of being restless, fidgety, and sometimes hyperactive in class, disrupting the environment and causing him many social problems. He would blurt out the answer at times and keep repeating it without any control, leading to some embarrassing timeouts. But he was always nice to his teachers, so he calls it a “benign frustration” rather than aggressively causing distress. He also talked about how his symptoms were dramatically improved with medication. Which of the following is an FDA approved drug for this patient’s most likely condition?
A 32-year-old man presents to the emergency department with vomiting, diarrhea, and abdominal pain 2 hours after eating seafood in a restaurant. He also mentions that immediately after ingestion of the food, he experienced tingling and numbness over the lips and face. On physical examination, his vital signs are stable. On neurological examination, he has reduced strength in the lower extremities, but deep tendon reflexes are present and normal. Laboratory evaluation of the seafood from the restaurant confirms the presence of a toxin which is known to block voltage-gated fast sodium channels. Which of the following toxins is the most likely cause of the patient’s symptoms?
A 44-year-old man presents to the clinic with recurrent epigastric pain following meals for a month. He adds that the pain radiates up his neck and throat. Over the counter antacids have not helped. On further questioning, he endorses foul breath upon waking in the morning and worsening of pain when lying down. He denies any recent weight loss. His temperature is 37°C (98.6°F), respirations are 15/min, pulse is 70/min, and blood pressure is 100/84 mm Hg. A physical examination is performed which is within normal limits except for mild tenderness on deep palpation of the epigastrium. An ECG performed in the clinic shows no abnormalities. What is the next best step in the management of this patient?
A 57-year-old man comes to the emergency department because of shortness of breath and palpitations for 3 hours. He has had similar episodes intermittently for 4 months. His pulse is 140/min and blood pressure is 90/60 mm Hg. An ECG shows irregular narrow-complex tachycardia with no discernable P waves. Emergent electrical cardioversion is performed and the patient reverts to normal sinus rhythm. Pharmacotherapy with sotalol is begun. Which of the following is the most likely physiologic effect of this drug?
A 54-year-old man electively underwent an open cholecystectomy for cholelithiasis. The procedure was performed under general anesthesia with inhaled anesthetic agents, including nitrous oxide, after induction with an intravenous agent. The surgeon operated quickly, and the procedure was uncomplicated. As the surgery ended, the anesthesia resident stopped the anesthesia and noticed the oxygen saturation gradually decreasing to 84%. He quickly administers 100% oxygen, and the hypoxia improves. Which of the following most likely accounts for the decreased oxygen saturation seen after the anesthesia was stopped in this patient?
A previously healthy 32-year-old man comes to the physician because of a 2-month history of fatigue and daytime sleepiness. He works as an accountant and cannot concentrate at work anymore. He also has depressed mood and no longer takes pleasure in activities he used to enjoy, such as playing tennis with his friends. He has decreased appetite and has had a 4-kg (8.8-lb) weight loss of over the past 2 months. He does not have suicidal ideation. He is diagnosed with major depressive disorder and treatment with paroxetine is begun. The patient is at greatest risk for which of the following adverse effects?
A 60-year-old man is brought to the emergency room because of fever and increasing confusion for the past 2 days. He has paranoid schizophrenia and hypertension. His current medications are chlorpromazine and amlodipine. He appears ill. He is not oriented to time, place, or person. His temperature is 40°C (104°F), pulse is 130/min, respirations are 29/min and blood pressure is 155/100 mm Hg. Examination shows diaphoresis. Muscle tone is increased bilaterally. Deep tendon reflexes are 1+ bilaterally. Neurologic examination shows psychomotor agitation. His speech is incoherent. Lungs are clear to auscultation. His neck is supple. The abdomen is soft and nontender. Serum laboratory analysis shows a leukocyte count of 11,300/mm3 and serum creatine kinase concentration of 833 U/L. Which of the following is the most appropriate initial pharmacotherapy?
A 42-year-old man is brought to the emergency department after having a seizure. His wife states that the patient has been struggling with alcohol abuse and has recently decided to "quit once and for all". Physical exam is notable for a malnourished patient responsive to verbal stimuli. He has moderate extremity weakness, occasional palpitations, and brisk deep tendon reflexes (DTRs). EKG demonstrates normal sinus rhythm and a prolonged QT interval. What nutritional deficiency most likely contributed to these findings?
A 65-year-old woman with COPD comes to the emergency department with 2-day history of worsening shortness of breath and cough. She often has a mild productive cough, but she noticed that her sputum is more yellow than usual. She has not had any recent fevers, chills, sore throat, or a runny nose. Her only medication is a salmeterol inhaler that she uses twice daily. Her temperature is 36.7°C (98°F), pulse is 104/min, blood pressure is 134/73 mm Hg, respiratory rate is 22/min, and oxygen saturation is 85%. She appears uncomfortable and shows labored breathing. Lung auscultation reveals coarse bibasilar inspiratory crackles. A plain film of the chest shows mild hyperinflation and flattening of the diaphragm but no consolidation. She is started on supplemental oxygen via nasal cannula. Which of the following is the most appropriate initial pharmacotherapy?
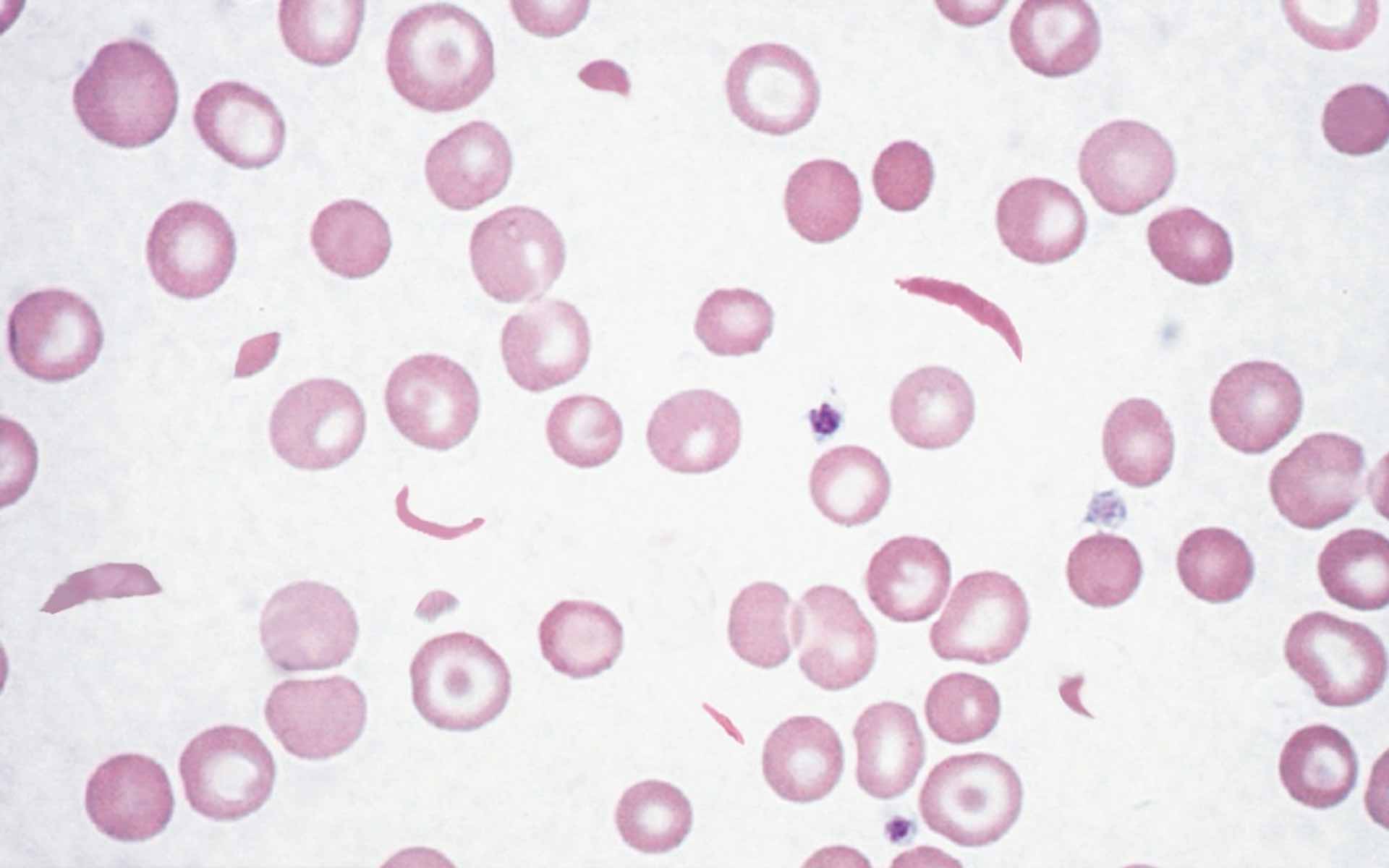
A 3-year-old boy is brought to the emergency department because of worsening pain and swelling in both of his hands for 1 week. He appears distressed. His temperature is 38.5°C (101.4°F). Examination shows erythema, swelling, warmth, and tenderness on the dorsum of his hands. His hemoglobin concentration is 9.1 g/dL. A peripheral blood smear is shown. The drug indicated to prevent recurrence of this patient's symptoms is also used to treat which of the following conditions?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app