
Autonomic/CV Drugs — MCQs

On this page
A 24-year-old woman in graduate school comes to the physician for recurrent headaches. The headaches are unilateral, throbbing, and usually preceded by blurring of vision. The symptoms last between 12 and 48 hours and are only relieved by lying down in a dark room. She has approximately two headaches per month and has missed several days of class because of the symptoms. Physical examination is unremarkable. The patient is prescribed an abortive therapy that acts by inducing cerebral vasoconstriction. Which of the following is the most likely mechanism of action of this drug?
A 38-year-old woman comes to the physician because of a 4-month history of crampy abdominal pain, recurrent watery diarrhea, and a 2.5-kg (5.5-lb) weight loss. Her husband has noticed that after meals, her face and neck sometimes become red, and she develops shortness of breath and starts wheezing. Examination shows a grade 3/6 systolic murmur heard best at the left lower sternal border. The abdomen is soft, and there is mild tenderness to palpation with no guarding or rebound. Without treatment, this patient is at greatest risk of developing which of the following conditions?
A 20-year-old man is found lying unconscious on the floor of his room by his roommate. The paramedics arrive at the site and find him unresponsive with cold, clammy extremities and constricted, non-reactive pupils. He smells of alcohol and his vital signs show the following: blood pressure 110/80 mm Hg, pulse 100/min, and respiratory rate 8/min. Intravenous access is established and dextrose is administered. The roommate suggests the possibility of drug abuse by the patient. He says he has seen the patient sniff a powdery substance, and he sees the patient inject himself often but has never confronted him about it. After the initial assessment, the patient is given medication and, within 5–10 minutes of administration, the patient regains consciousness and his breathing improves. He is alert and cooperative within the next few minutes. Which of the following drugs was given to this patient to help alleviate his symptoms?
A 65-year-old man presents to the physician with pain in his right calf over the last 3 months. He mentions that the pain typically occurs after he walks approximately 100 meters and subsides after resting for 5 minutes. His medical history is significant for hypercholesterolemia, ischemic heart disease, and bilateral knee osteoarthritis. His current daily medications include aspirin and simvastatin, which he has taken for the last 2 years. The physical examination reveals diminished popliteal artery pulses on the right side. Which of the following drugs is most likely to improve this patient's symptoms?
A 32-year-old woman brought to the emergency department because of a 1-week history of palpitations and shortness of breath. She has congestive heart failure. Current medications include furosemide, lisinopril, and atenolol. Her pulse is 124/min and irregularly irregular, and blood pressure is 110/70 mm Hg. Examination shows coarse crackles over the lower lung fields bilaterally. Treatment with digoxin is started. Five days later, an ECG shows prolongation of the PR interval. Which of the following is the most likely explanation for the observed effect of this drug?
A 2-year-old boy is brought to the physician for evaluation of delayed onset of speech. Over the past year, he has also had recurrent dizziness and three episodes of syncope. Examination of the ears shows clear auditory canals and intact tympanic membranes with normal light reflexes. Visual reinforcement audiometry shows bilateral sensorineural deafness. Genetic analysis reveals a mutation in the KCNQ1 gene causing a defect in slow voltage-gated potassium channels. An electrocardiogram of this patient is most likely to show which of the following?
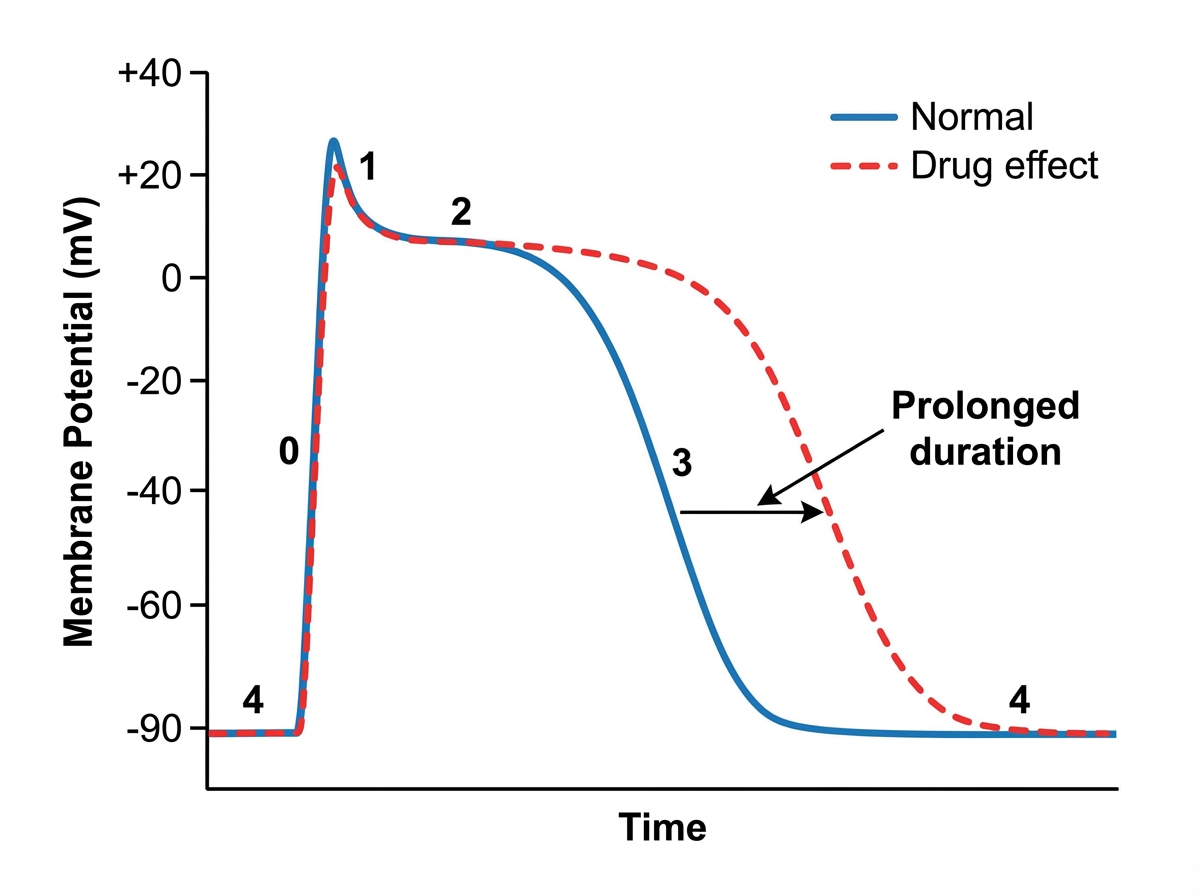
A 71-year-old woman comes to the physician because of dizziness and intermittent episodes of heart palpitations for 5 days. During this time, she has also had one episode of syncope. An ECG shows absence of P waves and irregular RR intervals. Treatment with an antiarrhythmic drug is initiated. The effect of the drug on the cardiac action potential is shown. Which of the following cardiac ion channels is most likely targeted by this drug?
A 45-year-old Caucasian male presents complaining of inability to open his mouth. Patient history reveals that he recently injured his foot from an exposed floor nail in his house. This patient's symptoms are likely the result of:
An 18-year-old college student presents to the ED straight from chemistry lab where he ingested an unknown compound. He complains of a headache, and is flushed, tachypneic and tachycardic. Suspecting cyanide poisoning, you administer amyl nitrite which causes which of the following?
A pharmaceutical company has created an experimental medication, Drug Z, for patients with relapsing-remitting multiple sclerosis. Drug Z has been deemed to be safe in rats and is nearly ready for human trials. Before initiating a Phase I clinical trial, the company would like to study the medication’s pharmacokinetic properties in humans. The drug was found to have a half-life of 2.5 hours and is eliminated by first-order kinetics. The volume of distribution of the drug is determined to be 0.5 L/kg. The drug is administered intravenously and sublingually and plasma drug concentration vs. time plots are obtained. Intravenous administration of 10 mg of Drug Z yields an area under the curve (AUC) of 15 mg hr/L. Sublingual administration of 25 mg of Drug Z yields an area under the curve of 20 mg hr/L. What is the absolute bioavailability of this medication?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app