
Autonomic/CV Drugs — MCQs

On this page
A 38-year-old man comes to the physician because of a 2-year-history of cough and progressively worsening breathlessness. He has smoked 1 pack of cigarettes daily for the past 10 years. Physical examination shows contraction of the anterior scalene and sternocleidomastoid muscles during inspiration. An x-ray of the chest shows flattening of the diaphragm and increased radiolucency in the lower lung fields. Further analysis shows increased activity of an isoform of elastase that is normally inhibited by alpha-1-antitrypsin. The cells that produce this isoform of elastase were most likely stimulated to enter the site of inflammation by which of the following substances?
A 10-year-old boy presents to the emergency department with sudden shortness of breath. He was playing in the school garden and suddenly started to complain of abdominal pain. He then vomited a few times. An hour later in the hospital, he slowly developed a rash on his chest, arms, and legs. His breathing became faster with audible wheezing. On physical examination, his vital signs are as follows: the temperature is 37.0°C (98.6°F), the blood pressure is 100/60 mm Hg, the pulse is 130/min, and the respiratory rate is 25/min. A rash is on his right arm, as shown in the image. After being administered appropriate treatment, the boy improves significantly, and he is able to breathe comfortably. Which of the following is the best marker that could be measured in the serum of this boy to help support the diagnosis?

A 17-year-old high school student is brought to the emergency department because of irritability and rapid breathing. He appears agitated and is diaphoretic. His temperature is 38.3°C (101°F), pulse is 129/min, respirations are 28/min, and blood pressure is 158/95 mmHg. His pupils are dilated. An ECG shows sinus tachycardia. Which of the following substances is used to make the drug this patient has most likely taken?
A 60-year-old man is brought to the emergency department because of a 30-minute history of dizziness and shortness of breath. After establishing the diagnosis, treatment with a drug is administered. Shortly after administration, the patient develops severe left eye pain and decreased vision of the left eye, along with nausea and vomiting. Ophthalmologic examination shows a fixed, mid-dilated pupil and a narrowed anterior chamber of the left eye. The patient was most likely treated for which of the following conditions?
A 33-year-old woman comes to the physician because of a 3-day history of dry cough and low-grade fever. Four months ago, she was diagnosed with major depressive disorder and started treatment with fluoxetine. Physical examination shows no abnormalities. A diagnosis of upper respiratory infection is made and medication is prescribed to relieve her symptoms. A drug with which of the following mechanisms of action should be avoided in this patient?
A 64-year-old man presents to his physician for a scheduled follow-up visit. He has chronic left-sided heart failure with systolic dysfunction. His current regular medications include captopril and digoxin, which were started after his last episode of symptomatic heart failure approximately 3 months ago. His last episode of heart failure was accompanied by atrial fibrillation, which followed an alcohol binge over a weekend. Since then he stopped drinking. He reports that he has no current symptoms at rest and is able to perform regular physical exercise without limitation. On physical examination, mild bipedal edema is noted. The physician suggested to him that he should discontinue digoxin and continue captopril and scheduled him for the next follow-up visit. Which of the following statements best justifies the suggestion made by the physician?
A 19-year-old G1P0 presents to the emergency department with severe abdominal pain. She states that the pain has been recurring every 3 to 5 minutes for the past 5 hours. She denies having regular prenatal care but recalls that her last menstrual period was about 9 months ago. She initially denies substance use but later admits to occasional prescription pain medication use during pregnancy. Her temperature is 98°F (37°C), blood pressure is 120/60 mmHg, pulse is 120/min, and respirations are 18/min. Tenderness is elicited in the lower abdominal quadrants. Clear fluid is seen in her vaginal vault with a fetal crown seen at 10 cm cervical dilation and +1 station. The patient is emergently taken into the labor and delivery suite, where she delivers a male infant with APGAR scores of 9 and 9 at 5 and 10 minutes, respectively. Several hours after delivery, the nurse notes that the infant is very irritable and crying in high pitches. The infant appears very diaphoretic with a runny nose and flailing limbs. What is the necessary pharmacological treatment for this patient?
A 25-year-old woman presents to the ED with nausea, vomiting, diarrhea, abdominal pain, and hematemesis after ingesting large quantities of a drug. Which of the following pairs a drug overdose with the correct antidote for this scenario?
A 48-year-old woman comes to the physician for a follow-up examination. At her visit 1 month ago, her glomerular filtration rate (GFR) was 100 mL/min/1.73 m2 and her renal plasma flow (RPF) was 588 mL/min. Today, her RPF is 540 mL/min and her filtration fraction (FF) is 0.2. After her previous appointment, this patient was most likely started on a drug that has which of the following effects?
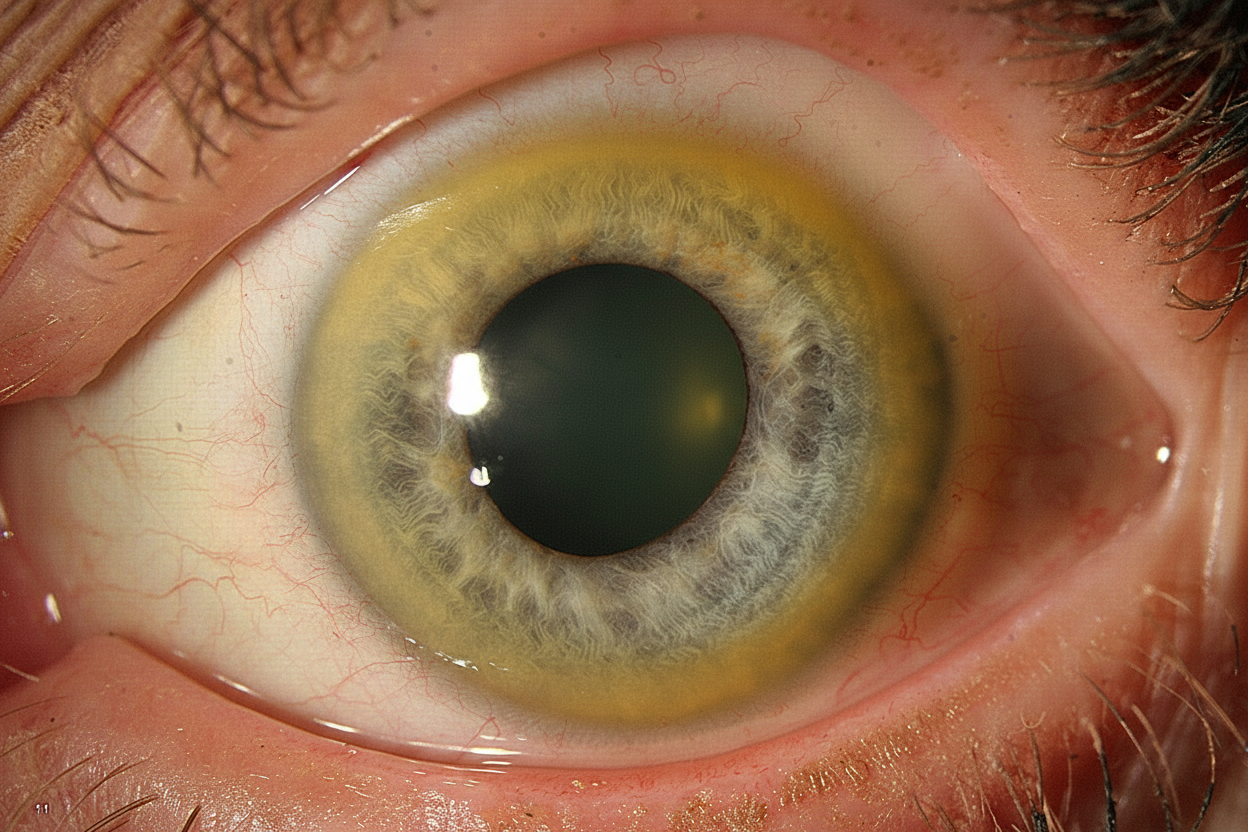
A 17-year-old man presents to his primary care physician with bilateral tremor of the hands. He is a senior in high school and during the year, his grades have plummeted to the point that he is failing. He says his memory is now poor, and he has trouble focusing on tasks. His behavior has changed in the past 6 months in that he has frequent episodes of depression, separated by episodes of bizarre behavior, including excessive alcohol drinking and shoplifting. His parents have started to suspect that he is using street drugs, which he denies. His handwriting has become very sloppy. His parents have noted slight slurring of his speech. Family history is irrelevant. Physical examination reveals upper extremity tremors, mild dystonia of the upper extremities, and mild incoordination involving his hands. The patient's eye is shown. Which of the following is the best initial management of this patient's condition?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app