
Autonomic/CV Drugs — MCQs

On this page
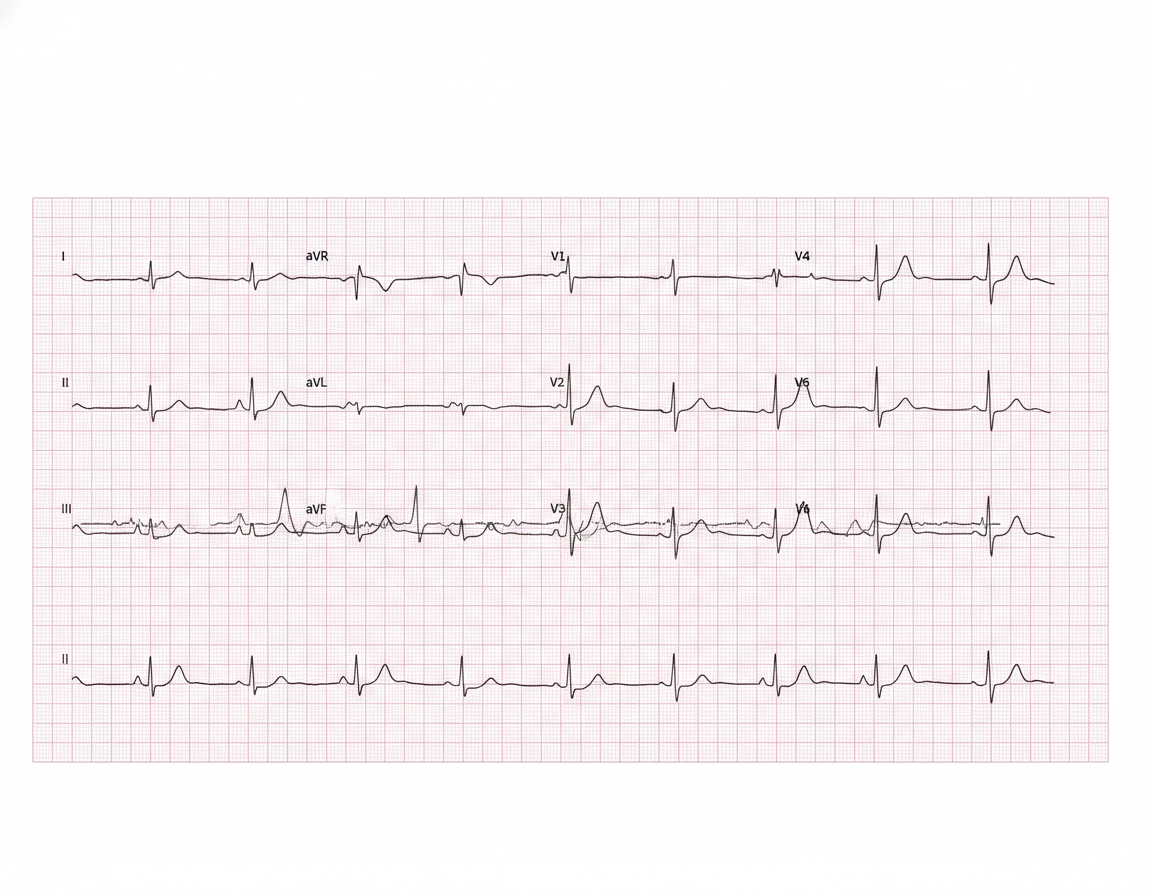
A 57-year-old man presents to the emergency department for evaluation of slurred speech and left arm and leg weakness over the last 3 hours. History reveals hypertension that is being treated with hydrochlorothiazide. Vital signs include: blood pressure of 110/70 mm Hg, heart rate 104/min, respiratory rate 18/min, and temperature 36.6°C (98.0°F). Physical examination reveals 2/5 strength in both left upper and lower extremities. After 2 hours, the patient's symptoms suddenly disappear. An electrocardiogram (ECG) is obtained (see image). Which of the following medications could prevent ischemic attacks in this patient in the future?
A 66-year-old man is brought to the emergency department 1 hour after the abrupt onset of painless loss of vision in his left eye. Over the last several years, he has noticed increased blurring of vision; he says the blurring has made it difficult to read, but he can read better if he holds the book below or above eye level. He has smoked 1 pack of cigarettes daily for 40 years. Fundoscopic examination shows subretinal fluid and small hemorrhage with grayish-green discoloration in the macular area in the left eye, and multiple drusen in the right eye with retinal pigment epithelial changes. Which of the following is the most appropriate pharmacotherapy for this patient's eye condition?
A 35-year-old woman presents to the clinic with a 2-week history of headaches. She was in her usual state of health until 2 weeks ago, when she started having headaches. The headaches are throughout her whole head and rated as a 7/10. They are worse in the mornings and when she bends over. She has some mild nausea, but no vomiting. The headaches are not throbbing and are not associated with photophobia or phonophobia. On further questioning, she has noticed more hair than usual on her pillow in the morning and coming out in her hands when she washes her hair. The past medical history is unremarkable; she takes no prescription medications, but for the past year she has been taking an oral 'health supplement' recommended by her sister, which she orders over the internet. She cannot recall the supplement's name and does not know its contents. The physical exam is notable for some mild hepatomegaly but is otherwise unremarkable. This patient's presentation is most likely related to which of the following micronutrients?
A 22-year-old woman with type 1 diabetes mellitus and mild asthma comes to the physician for a follow-up examination. She has had several episodes of sweating, dizziness, and nausea in the past 2 months that occur during the day and always resolve after she drinks orange juice. She is compliant with her diet and insulin regimen. The physician recommends lowering her insulin dose in certain situations. This recommendation is most important in which of the following situations?
A 25-year-old man presents to the emergency department with pain in his leg. He states that the pain was sudden and that his leg feels very tender. This has happened before, but symptoms resolved a few days later with acetaminophen. His temperature is 98.5°F (36.9°C), blood pressure is 129/88 mmHg, pulse is 90/min, respirations are 12/min, and oxygen saturation is 98% on room air. Physical exam reveals clear breath sounds bilaterally and a normal S1 and S2. The patient’s right leg is red, inflamed, and tender to palpation inferior to the popliteal fossa. Which of the following is the best treatment for this patient?
A 42-year-old man is brought in to the emergency department by his daughter. She reports that her father drank heavily for the last 16 years, but he stopped 4 days ago after he decided to quit drinking on his birthday. She also reports that he has been talking about seeing cats running in his room since this morning, although there were no cats. There is no history of any known medical problems or any other substance use. On physical examination, his temperature is 38.4ºC (101.2ºF), heart rate is 116/min, blood pressure is 160/94 mm Hg, and respiratory rate is 22/min. He is severely agitated and is not oriented to his name, time, or place. On physical examination, profuse perspiration and tremors are present. Which of the following best describes the pathophysiologic mechanism underlying his condition?
A 47-year-old African-American woman presents to her primary care physician for a general checkup appointment. She works as a middle school teacher and has a 25 pack-year smoking history. She has a body mass index (BMI) of 22 kg/m^2 and is a vegetarian. Her last menstrual period was 1 week ago. Her current medications include oral contraceptive pills. Which of the following is a risk factor for osteoporosis in this patient?
A 33-year-old man comes to the emergency department because of a pounding headache for the past 3 hours. The pain is 8 out of 10 in intensity, does not radiate, and is not relieved by ibuprofen. He also has associated dizziness, blurring of vision, and palpitations. He has had similar episodes over the last 6 months but none this severe. He has not had fever, weight change, or loss of appetite. He underwent an appendectomy at the age of 18. His father died of renal cancer. He is diaphoretic. His temperature is 36.8°C (98.4°F), pulse is 112/min, and blood pressure is 220/130 mm Hg. Physical examination shows no abnormalities. Laboratory studies show: Hemoglobin 14.8 g/dL Leukocyte count 9600/mm3 Platelet count 345,000/mm3 Serum Glucose 112 mg/dL Na+ 137 mEq/L K+ 4.2 mEq/L Cl- 105 mEq/L Creatinine 1.0 mg/dL Urine dipstick shows no abnormalities. Which of the following findings on imaging is the most likely explanation for this patient's symptoms?
A 25-year-old man presents to the clinic with a complaint of lightheadedness when standing up from his bed in the morning and then from his chair at work. He has had similar complaints for many months, and the symptoms have not improved despite drinking lots of fluids, eating regular meals, and taking daily multivitamin. His daily routine is disturbed as he finds himself getting up very slowly to avoid the problem. This has created some awkward situations at his workplace and in social settings. His blood pressure while seated is 120/80 mm Hg, and upon standing it falls to 100/68 mm Hg. The physical examination is unremarkable except for a strong odor suggestive of marijuana use. The patient denies drug use and insists the odor is due to his roommate who smokes marijuana for medical purposes. No pallor or signs of dehydration are seen. The lab results are as follows: Serum Glucose 90 mg/dL Sodium 140 mEq/L Potassium 4.1 mEq/L Chloride 100 mEq/L Serum Creatinine 0.8 mg/dL Blood Urea Nitrogen 9 mg/dL Hemoglobin (Hb) Concentration 15.3 g/dL Mean Corpuscular Volume (MCV) 83 fl Reticulocyte count 0.5% Erythrocyte count 5.3 million/mm3 Platelet count 200,000/mm3 The ECG shows no abnormal finding. Which of the following could alleviate this patient’s symptoms?
A 7-year-old boy with asthma is brought to the physician because of a 1-month history of worsening shortness of breath and cough. The mother reports that the shortness of breath usually occurs when he is exercising with his older brother. His only medication is an albuterol inhaler that is taken as needed. The physician considers adding zafirlukast to his drug regimen. Which of the following is the most likely mechanism of action of this drug?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app