
Autonomic/CV Drugs — MCQs

On this page
A 56-year-old man presents for a follow-up regarding his management for type 2 diabetes mellitus (DM). He was diagnosed with type 2 DM about 7 years ago and was recently started on insulin therapy because oral agents were insufficient to control his glucose levels. He is currently following a regimen combining insulin lispro and neutral protamine Hagedorn (NPH) insulin. He is taking insulin lispro 3 times a day before meals and NPH insulin once in the morning. He has been on this regimen for about 2 months. He says that his glucose reading at night averages around 200 mg/dL and remains close to 180 mg/dL before his shot of NPH in the morning. The readings during the rest of the day range between 100–120 mg/dL. The patient denies any changes in vision or tingling or numbness in his hands or feet. His latest HbA1C level was 6.2%. Which of the following adjustments to his insulin regimen would be most effective in helping this patient achieve better glycemic control?
A 52-year-old man who was recently hospitalized with a pulmonary embolism is put on an unfractionated heparin drip as a bridge to chronic warfarin therapy. During morning rounds, he is found to have diffuse bruising despite minimal trauma, and his heparin infusion rate is found to be faster than prescribed. A coagulation panel is obtained, which shows a aPTT of 130 seconds (therapeutic 70-120 seconds), and the decision is made to reverse the effects of heparin. Which of the following would most likely be administered in order to do this?
Background: Beta-blockers reduce mortality in patients who have chronic heart failure, systolic dysfunction, and are on background treatment with diuretics and angiotensin-converting enzyme inhibitors. We aimed to compare the effects of carvedilol and metoprolol on clinical outcome. Methods: In a multicenter, double-blind, and randomized parallel group trial, we assigned 1,511 patients with chronic heart failure to treatment with carvedilol (target dose 25 mg twice daily) and 1,518 to metoprolol (metoprolol tartrate, target dose 50 mg twice daily). Patients were required to have chronic heart failure (NYHA II-IV), previous admission for a cardiovascular reason, an ejection fraction of less than 0.35, and to have been treated optimally with diuretics and angiotensin-converting enzyme inhibitors unless not tolerated. The primary endpoints were all-cause mortality, the composite endpoint of all-cause mortality, or all-cause admission. Analysis was done by intention to treat Findings: The mean study duration was 58 months (SD 6). The mean ejection fraction was 0.26 (0.07) and the mean age was 62 years (11). The all-cause mortality was 34% (512 of 1,511) for carvedilol and 40% (600 of 1,518) for metoprolol (hazard ratio 0.83 [95% CI 0.74-0.93], p = 0.0017). The reduction of all-cause mortality was consistent across predefined subgroups. Incidence of side effects and drug withdrawals did not differ by much between the 2 study groups. Which of the following represents the number of patients needed to treat to save one life?
A 56-year-old man presents with sudden-onset severe eye pain and blurred vision. He says the symptoms onset an hour ago and his vision has progressively worsened. Physical examination reveals a cloudy cornea and decreased visual acuity. Timolol is administered into the eyes to treat this patient’s symptoms. Which of the following best describes the mechanism of action of this drug in the treatment of this patient’s condition?
A 48-year-old woman underwent a thyroidectomy with central neck dissection due to papillary thyroid carcinoma. On day 2 postoperatively, she developed irritability, dysphagia, difficulty breathing, and spasms in different muscle groups in her upper and lower extremities. The vital signs include blood pressure 102/65 mm Hg, heart rate 93/min, respiratory rate 17/min, and temperature 36.1℃ (97.0℉). Physical examination shows several petechiae on her forearms, muscle twitching in her upper and lower extremities, expiratory wheezes on lung auscultation, decreased S1 and S2 and the presence of an S3 on cardiac auscultation, and positive Trousseau and Chvostek signs. Laboratory studies show: Ca2+ 4.4 mg/dL Mg2+ 1.7 mEq/L Na+ 140 mEq/L K+ 4.3 mEq/L Cl- 107 mEq/L HCO3- 25 mEq/L Administration of which of the following agents could prevent the patient’s condition?
A 25-year-old man presents to the emergency department after a motor vehicle accident. He was the unrestrained front seat driver in a head on collision. The patient is unresponsive and his medical history is unknown. His temperature is 99.5°F (37.5°C), blood pressure is 67/38 mmHg, pulse is 190/min, respirations are 33/min, and oxygen saturation is 98% on room air. The patient is started on IV fluids, blood products, and norepinephrine. A FAST exam is performed and a pelvic binder is placed. One hour later, his temperature is 98.3°F (36.8°C), blood pressure is 119/66 mmHg, pulse is 110/min, respirations are 15/min, and oxygen saturation is 97% on room air. The patient is currently responsive. Management of the patient's pelvic fracture is scheduled by the orthopedic service. While the patient is waiting in the emergency department he suddenly complains of feeling hot, aches, and a headache. The patient's temperature is currently 101°F (38.3°C). He has not been given any pain medications and his past medical history is still unknown. Which of the following is the most likely diagnosis?
A 16-year-old boy with history of seizure disorder is rushed to the Emergency Department with multiple generalized tonic-clonic seizures that have spanned more than 30 minutes in duration. He has not regained consciousness between these episodes. In addition to taking measures to ensure that he maintains adequate respiration, which of the following is appropriate for initial pharmacological therapy?
A 60-year-old male presents to the emergency room complaining of substernal chest pain. He reports a three-hour history of dull substernal chest pain that radiates into his left arm and jaw. He had a similar incident two months ago after walking one mile, but this pain is more severe. His past medical history is notable for hypertension and hyperlipidemia. An EKG demonstrates non-specific changes. Serum troponins are normal. In addition to aspirin, oxygen, and morphine, he is started on a medication that releases nitric oxide. Which of the following is a downstream effect of this molecule?
A 5-year-old boy undergoes MRI neuroimaging for the evaluation of worsening headaches and intermittent nausea upon awakening. He receives a bolus of intravenous thiopental for sedation during the procedure. Ten minutes after the MRI, the patient is awake and responsive. Which of the following pharmacological properties is most likely responsible for this patient's rapid recovery from this anesthetic agent?
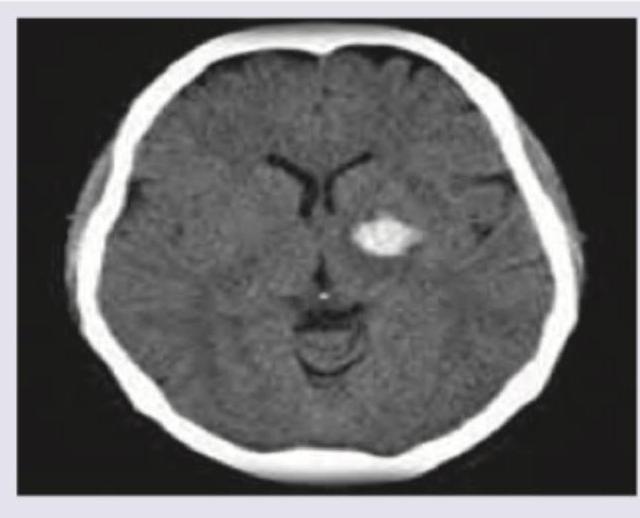
A 70-year-old Caucasian male presents to the emergency room following a fall. The patient's past medical history is significant for myocardial infarction and atrial fibrillation. His home medications are unknown. The patient's head CT is shown in Image A. Laboratory results reveal an International Normalized Ratio (INR) of 6. Which of the following is the most appropriate pharmacologic therapy for this patient?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app