
Autonomic/CV Drugs — MCQs

On this page
A 63-year-old man presents to his primary care provider with colicky pain radiating to his left groin. The pain has been intermittent for several days. He has also been experiencing occasional burning pain in his hands and feet and frequent headaches. His past medical history is significant for an NSTEMI last year. He is currently taking atorvastatin and low dose aspirin. Today his temperature is 36.8°C (98.2°F), the heart rate is 103/min, the respiratory rate is 15/min, the blood pressure 135/85 mm Hg, and the oxygen saturation is 100% on room air. On physical exam, he appears gaunt and anxious. His heart is tachycardia with a regular rhythm and his lungs are clear to auscultation bilaterally. On abdominal exam he has hepatomegaly. A thorough blood analysis reveals a hemoglobin of 22 mg/dL and a significantly reduced EPO. Renal function and serum electrolytes are within normal limits. A urinalysis is positive for blood. A non-contrast CT shows a large kidney stone obstructing the left ureter. The patient’s pain is managed with acetaminophen and the stone passes with adequate hydration. It is sent to pathology for analysis. Additionally, a bone marrow biopsy is performed which reveals trilineage hematopoiesis and hypercellularity with a JAK2 mutation. Which medication would help prevent future episodes of nephrolithiasis?
A 59-year-old woman is referred to a neurologist for a hand tremor. Her symptoms began a few months prior to presentation and has progressively worsened. She noticed she was having difficulty drinking her coffee and writing in her notebook. The patient reports that her father also had a tremor but is unsure what type of tremor it was. She drinks 2-3 glasses of wine per week and only takes a multivitamin. Laboratory studies prior to seeing the neurologist demonstrated a normal basic metabolic panel and thyroid studies. On physical exam, there is a mid-amplitude 8 Hz frequency postural tremor of the right hand. The tremor is notable when the right hand is outstretched to the very end of finger-to-nose testing. Neurologic exam is otherwise normal. Which of the following is the best treatment option for this patient?
A 51-year-old woman with a history of paroxysmal atrial fibrillation comes to the physician for a follow-up visit. She feels well and wants to discuss pausing her only current medication, flecainide. Her pulse is 75/min and regular, blood pressure is 125/75 mm Hg. Physical examination shows no abnormalities. An ECG shows a PR interval of 180 ms, QRS time of 120 ms, and corrected QT interval of 440 ms. Which of the following ECG changes is most likely to be seen on cardiac stress testing in this patient?
A 31-year-old male with bipolar disorder comes to the physician because of erectile dysfunction for the past month. He cannot maintain an erection during intercourse and rarely wakes up with an erection. He says he is happy in his current relationship, but admits to decreased desire for sex and feeling embarrassed about his sexual performance. He sustained a lumbar vertebral injury one year ago following a motor vehicle accident. He takes medication for his bipolar disorder but does not remember the name. Physical examination shows testicular atrophy with otherwise normal genitalia. Which of the following is the most likely cause of this patient's symptoms?
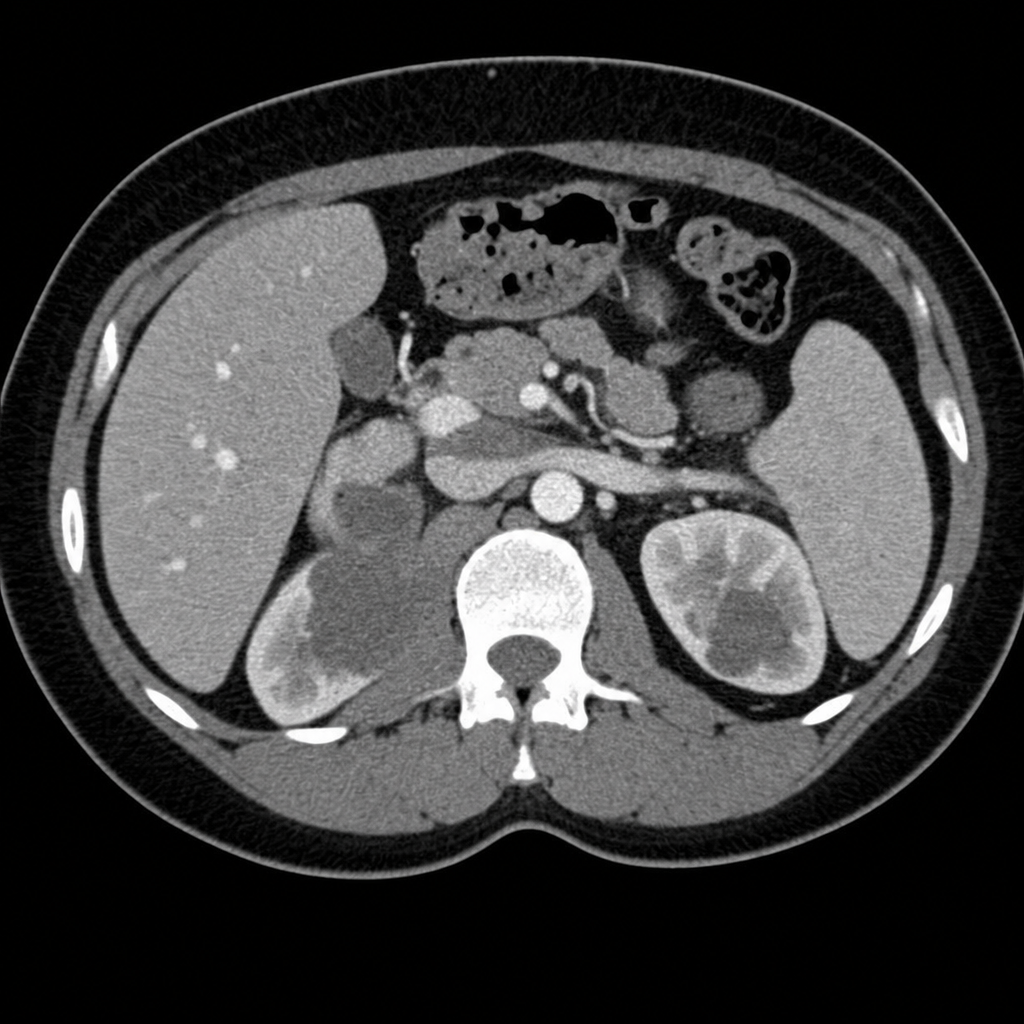
A 30-year-old woman presents to her primary care provider with blood in her urine and pain in her left flank. She has a 5-year history of polycystic ovarian syndrome managed with oral contraceptives and metformin. She is single and is not sexually active and denies a history of kidney stones or abdominal trauma. She has a 15-pack-year smoking history but denies the use of other substances. Her family history is significant for fatal lung cancer in her father at age 50, who also smoked, and recently diagnosed bladder cancer in her 45-year-old brother, who never smoked. On review of systems, she denies weight loss, fever, fatigue, paresthesia, increased pain with urination, or excessive bleeding or easy bruising. She is admitted to the hospital for a workup and observation. Her vital signs and physical exam are within normal limits. A urine pregnancy test is negative. PT is 14 sec and PTT is 20 sec. The rest of the laboratory results including von Willebrand factor activity and lupus anticoagulant panel are pending. A CT angiogram is ordered and is shown in the picture. What is indicated at this time to prevent a potential sequela of this patient's condition?
A 23-year-old man comes to the emergency department because of a rash on his neck and back for the past 6 hours. He says that he first noticed some reddening of the skin on his back the previous evening, which turned into a blistering, red rash overnight. He went surfing the previous day and spent 5 hours at the beach. He reports having applied at least 1 oz of water-resistant SPF 30 sunscreen 30 minutes before leaving his home. His vitals are within normal limits. Physical examination shows erythema of the skin over the upper back and dorsum of the neck, with 3 vesicles filled with clear fluid. The affected area is edematous and tender to touch. Which of the following recommendations is most appropriate to prevent a recurrence of this patient's symptoms in the future?
A 58-year-old woman presents to the office after receiving a bone mineral density screening test result with a T score of -4.1 and a Z score of -3.8. She is diagnosed with osteoporosis. A review of her medical history reveals that she has taken estrogen-containing oral contraceptive pills from the age of 20 to 30. She suffered from heartburn from the age of 45 and took lansoprazole and ranitidine often for her symptoms. She also was on lithium for 2 years after being diagnosed with bipolar disorder at the age of 54. Last year she was diagnosed with congestive heart failure and was started on low dose hydrochlorothiazide. Which of her medications most likely contributed to the development of her osteoporosis?
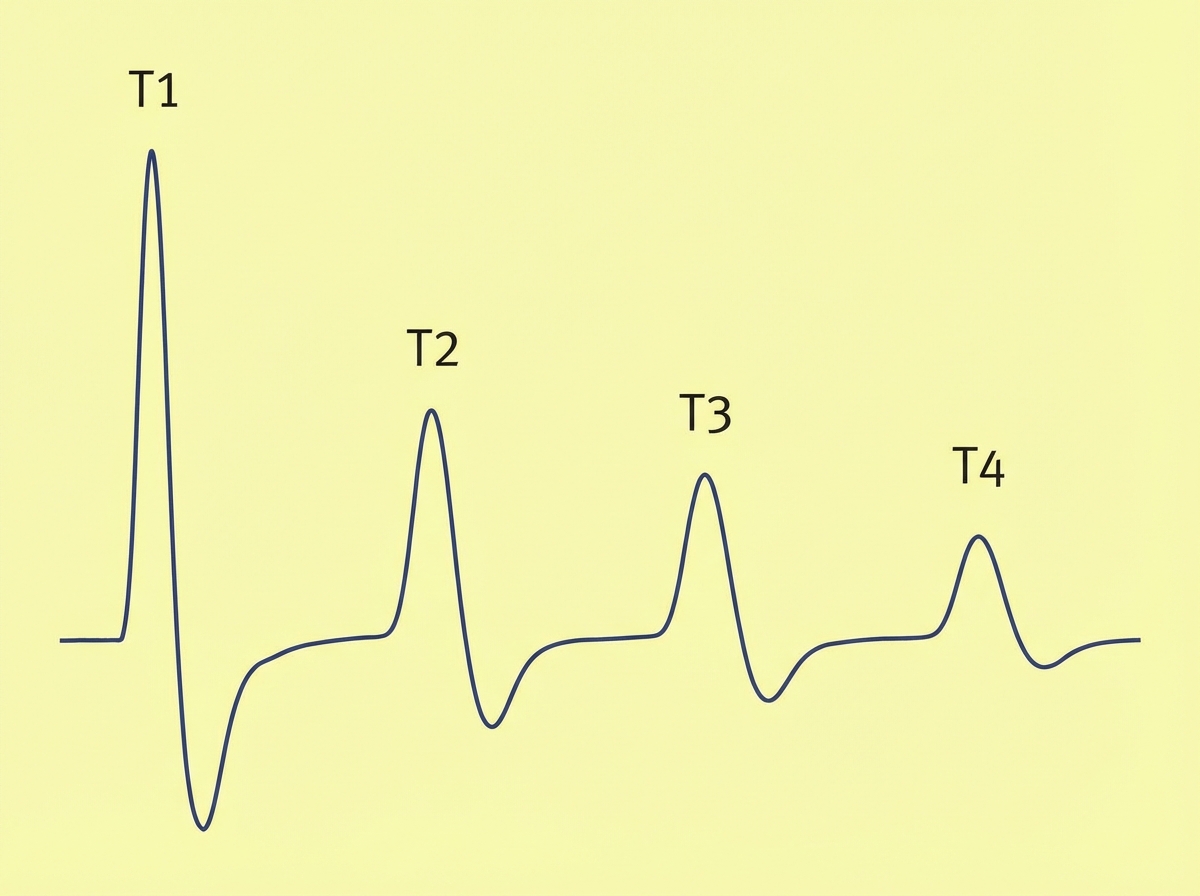
A 37-year-old woman undergoes diagnostic laparoscopy under general anesthesia for evaluation of chronic pelvic pain. Postoperatively, the patient requires prolonged intubation. Neostigmine is administered. Results of acceleromyography during train-of-four ulnar nerve stimulation are shown. Which of the following drugs is most likely to have been used intraoperatively in this patient?
A 56-year-old man comes to the physician because of a painless blistering rash on his hands, forearms, and face for 2 weeks. The rash is not itchy and seems to get worse in the sunlight. He has also noticed that his urine is darker than usual. His aunt and sister have a history of similar skin lesions. Examination of the skin shows multiple fluid-filled blisters and oozing erosions on the forearms, dorsal side of both hands, and forehead. There are areas of hyperpigmented scarring and patches of bald skin along the sides of the blisters. Which of the following is the most appropriate pharmacotherapy to treat this patient's condition?
A 57-year-old man presents to his family physician for a checkup. He has had type 2 diabetes mellitus for 13 years, for which he has been taking metformin and vildagliptin. He has smoked 10–15 cigarettes daily for 29 years. Family history is irrelevant. Vital signs include: temperature 36.6°C (97.8°F), blood pressure 152/87 mm Hg and pulse 88/min. Examination reveals moderate abdominal obesity with a body mass index of 32 kg/m². The remainder of the examination is unremarkable. His fasting lipid profile is shown: Total cholesterol (TC) 280 mg/dL Low-density lipoprotein (LDL)-cholesterol 210 mg/dL High-density lipoprotein (HDL)-cholesterol 40 mg/dL Triglycerides (TGs) 230 mg/dL Which of the following is the mechanism of action of the best initial therapy for this patient?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app