
Autonomic/CV Drugs — MCQs

On this page
A 42-year-old woman comes to the physician for evaluation of a 6-month history of irregular menstrual periods. Her last period was 3 months ago. Previously, her periods occurred at regular 28-day intervals and lasted 4–5 days with moderate flow. She has also noticed breast tenderness and scant nipple discharge. She has type 2 diabetes mellitus and refractory bipolar I disorder. Current medications include metformin, glipizide, lithium, and risperidone. Physical examination shows no abnormalities. A urine pregnancy test is negative. Which of the following is the most likely cause of the changes in her menstrual cycle?
A 65-year-old gentleman presents to his primary care physician for difficulties with his gait and recent fatigue. The patient works in a health food store, follows a strict vegan diet, and takes an array of supplements. He noticed that his symptoms have progressed over the past year and decided to see a physician when he found himself feeling abnormally weak on a daily basis in conjunction with his trouble walking. The patient has a past medical history of Crohn's disease, diagnosed in his early 20's, as well as Celiac disease. He states that he has infrequent exacerbations of his Crohn's disease. Recently, the patient has been having worsening bouts of diarrhea that the patient claims is non-bloody. The patient is not currently taking any medications and is currently taking traditional Chinese medicine supplements. Physical exam is notable for 3/5 strength in the upper and lower extremities, absent upper and lower extremity reflexes, and a staggering, unbalanced gait. Laboratory values reveal the following: Serum: Na+: 135 mEq/L Cl-: 100 mEq/L K+: 5.6 mEq/L HCO3-: 22 mEq/L BUN: 27 mg/dL Glucose: 79 mg/dL Creatinine: 1.1 mg/dL Ca2+: 8.4 mg/dL Mg2+: 1.5 mEq/L Leukocyte count and differential: Leukocyte count: 4,522/mm^3 Hemoglobin: 9.2 g/dL Hematocrit: 29% Platelet count: 169,000/mm^3 Reticulocyte count: 2.5% Lactate dehydrogenase: 340 U/L Mean corpuscular volume: 97 fL Which of the following is most likely deficient in this patient?
A 55-year-old woman comes to the clinic complaining of joint pain and stiffness for the past year. The pain is mainly concentrated in her hands and is usually worse towards the late afternoon. It is described with a burning quality that surrounds the joint with some numbness and tingling. The stiffness is especially worse in the morning and lasts approximately for 15-20 minutes. Her past medical history is significant for recurrent gastric ulcers. She reports that her mother struggled with lupus and is concerned that she might have the same thing. She denies fever, rashes, ulcers, genitourinary symptoms, weight loss, or bowel changes. Physical examination is significant for mild tenderness at the distal interphalangeal joints bilaterally. What is the best initial medication to prescribe to this patient?
A 36-year-old woman comes to the physician because of multiple episodes of headache over the past 3 months. The headaches last the entire day and are unilateral and throbbing. During the headaches, she has severe nausea and is unable to work and perform her daily activities. She has noticed that she becomes unusually hungry prior to the onset of headache. She locks herself in a dark room, takes ibuprofen, and avoids going out until the headache subsides. However, over the past month, the headaches have increased to 2–3 times a week and become more intense. She has hypertension treated with amlodipine. Her temperature is 37°C (98.6°F), pulse is 80/min, and blood pressure is 128/76 mm Hg. Physical and neurologic examinations show no abnormalities. Which of the following is the most appropriate therapy for long-term prevention of headaches in this patient?
A 57-year-old man is brought to the emergency department 2 hours after the onset of severe nausea and vomiting. He also has cramping abdominal pain and feels fatigued. Two months ago, he injured his lumbar spine in a car accident and lost complete motor and sensory function below the level of injury. He has been bedridden ever since and is cared for at home. He has type 2 diabetes mellitus and renal insufficiency. Examination shows dry mucosal membranes and sensory impairment with flaccid paralysis in both lower limbs that is consistent with prior examinations. Laboratory studies show: Serum Calcium 12.8 mg/dL Parathyroid hormone, N-terminal 180 pg/mL Thyroid-stimulating hormone 2.5 μU/mL Thyroxine 8 μg/dL Calcitriol Decreased Creatinine 2.6 mg/dL Urine Calcium 550 mg/24 h In addition to administration of intravenous 0.9% saline and calcitonin, which of the following is the most appropriate next step in management?
A 24-year-old graduate student is brought to the emergency department by her boyfriend because of chest pain that started 90 minutes ago. Her boyfriend says she has been taking medication to help her study for an important exam and has not slept in several days. On examination, she is diaphoretic, agitated, and attempts to remove her IV lines and ECG leads. Her temperature is 37.6°C (99.7°F), pulse is 128/min, and blood pressure is 163/97 mmHg. Her pupils are dilated. The most appropriate next step in management is the administration of which of the following?
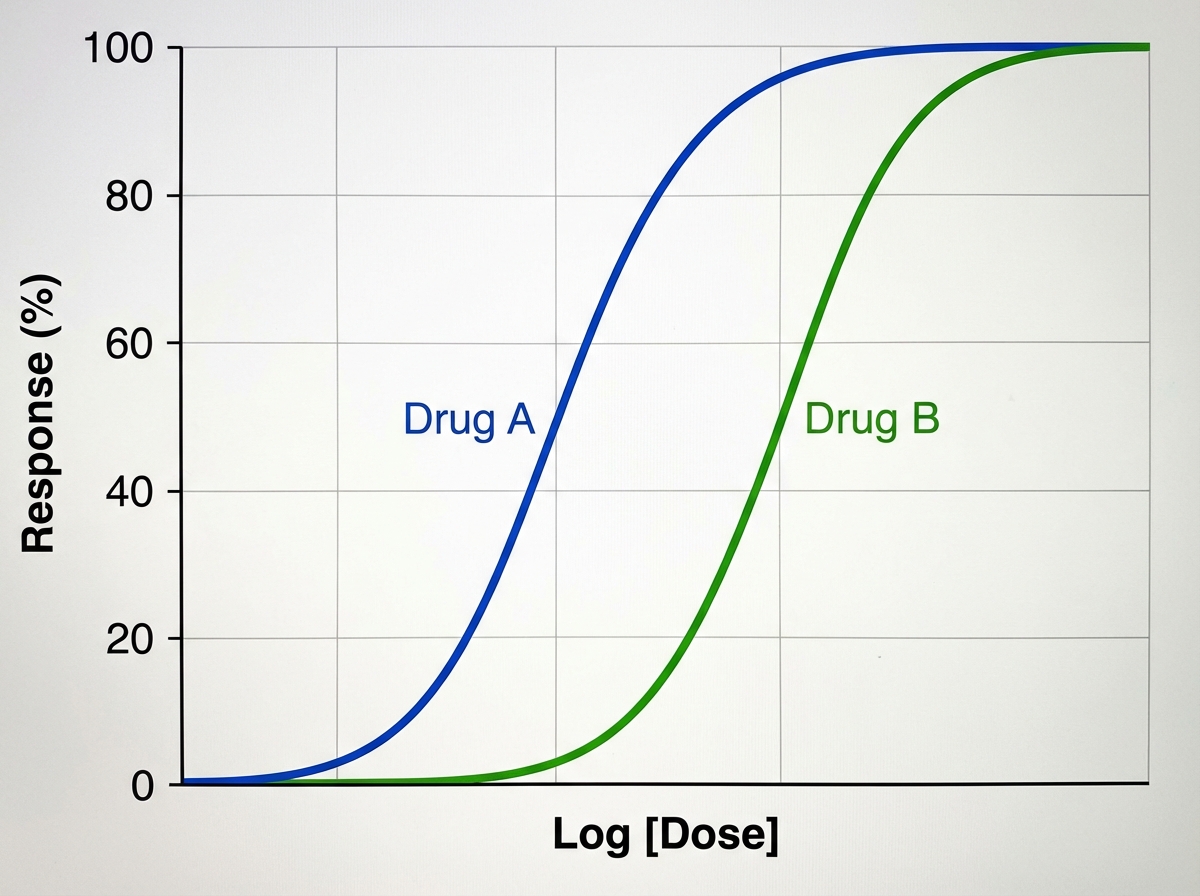
A medical student is reviewing dose-response curves of various experimental drugs. She is specifically interested in the different factors that cause the curve to shift in different directions. From her study, she plots the following graph (see image). She marks the blue curve for drug A, which acts optimally on a receptor. After drawing the second (green) curve for drug B, she discovers that more of drug B is required to produce the same response as drug A, although drug B can still achieve the same maximum effect. Which of the following terms best describes the activity of drug B in comparison to drug A?
A 71-year-old woman presents to her hematologist-oncologist for follow up after having begun doxorubicin and cyclophosphamide in addition to radiation therapy for the treatment of her stage 3 breast cancer. Her past medical history is significant for preeclampsia, hypertension, polycystic ovarian syndrome, and hypercholesterolemia. She currently smokes 1 pack of cigarettes per day, drinks a glass of wine per day, and denies any illicit drug use. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 111/min, and respiratory rate 23/min. On physical examination, the pulses are strong and irregular, she has a grade 3/6 holosystolic murmur heard best at the left upper sternal border, clear bilateral breath sounds, and erythema over her site of radiation. Which of the following statements regarding doxorubicin is true?
A 70-year-old man comes to the physician for a follow-up examination of diffuse exertional chest pain which he has successfully been treating with sublingual nitroglycerin for the past year. The patient has been taking lisinopril daily for essential hypertension. His pulse is 75/min and regular, and blood pressure is 155/90 mm Hg. Cardiac and pulmonary examination show no abnormalities; there is no peripheral edema. A decrease of which of the following is the most likely explanation for the improvement of this patient's chest pain?
A previously healthy 8-year-old boy is brought to the physician by his mother because of 6 months of progressive fatigue and weight loss. His mother reports that during this time, he has had decreased energy and has become a “picky eater.” He often has loose stools and complains of occasional abdominal pain and nausea. His family moved to a different house 7 months ago. He is at the 50th percentile for height and 25th percentile for weight. His temperature is 36.7°C (98°F), pulse is 116/min, and blood pressure is 85/46 mm Hg. Physical examination shows tanned skin and bluish-black gums. The abdomen is soft, nondistended, and nontender. Serum studies show: Na+ 134 mEq/L K+ 5.4 mEq/L Cl- 104 mEq/L Bicarbonate 21 mEq/L Urea nitrogen 16 mg/dL Creatinine 0.9 mg/dL Glucose 70 mg/dL Intravenous fluid resuscitation is begun. Which of the following is the most appropriate initial step in treatment?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app