
Autonomic/CV Drugs — MCQs

On this page
A 54-year-old man comes to the emergency department because of episodic palpitations for the past 12 hours. He has no chest pain. He has coronary artery disease and type 2 diabetes mellitus. His current medications include aspirin, insulin, and atorvastatin. His pulse is 155/min and blood pressure is 116/77 mm Hg. Physical examination shows no abnormalities. An ECG shows monomorphic ventricular tachycardia. An amiodarone bolus and infusion is given, and the ventricular tachycardia converts to normal sinus rhythm. He is discharged home with oral amiodarone. Which of the following is the most likely adverse effect associated with long-term use of this medication?
A 34-year-old female presents to the emergency room with headache and palpitations. She is sweating profusely and appears tremulous on exam. Vital signs are as follows: HR 120, BP 190/110, RR 18, O2 99% on room air, and Temp 37C. Urinary metanephrines and catechols are positive. Which of the following medical regimens is contraindicated as a first-line therapy in this patient?
A 3-year-old toddler was rushed to the emergency department after consuming peanut butter crackers at daycare. The daycare staff report that the patient has a severe allergy to peanut butter and he was offered the crackers by mistake. The patient is in acute distress. The vital signs include: blood pressure 60/40 mm Hg and heart rate 110/min. There is audible inspiratory stridor and the respiratory rate is 27/min. Upon examination, his chest is covered in a maculopapular rash. Intubation is attempted and failed due to extensive laryngeal edema. The decision for cricothyrotomy is made. Which of the following is the most likely mechanism of this pathology?
A 59-year-old healthy woman presents to her primary care physician’s office six weeks after undergoing an elective breast augmentation procedure in the Dominican Republic. She was told by her surgeon to establish post-operative care once back in the United States. Today she is bothered by nausea and early satiety. Her past medical history is significant only for GERD for which she takes ranitidine. Since the surgery, she has also taken an unknown opioid pain medication that was given to her by the surgeon. She reports that she has been taking approximately ten pills a day. On examination she is afebrile with normal vital signs and her surgical incisions are healing well. Her abdomen is distended and tympanitic. The patient refuses to stop her pain medicine and laxatives are not effective; what medication could be prescribed to ameliorate her gastrointestinal symptoms?
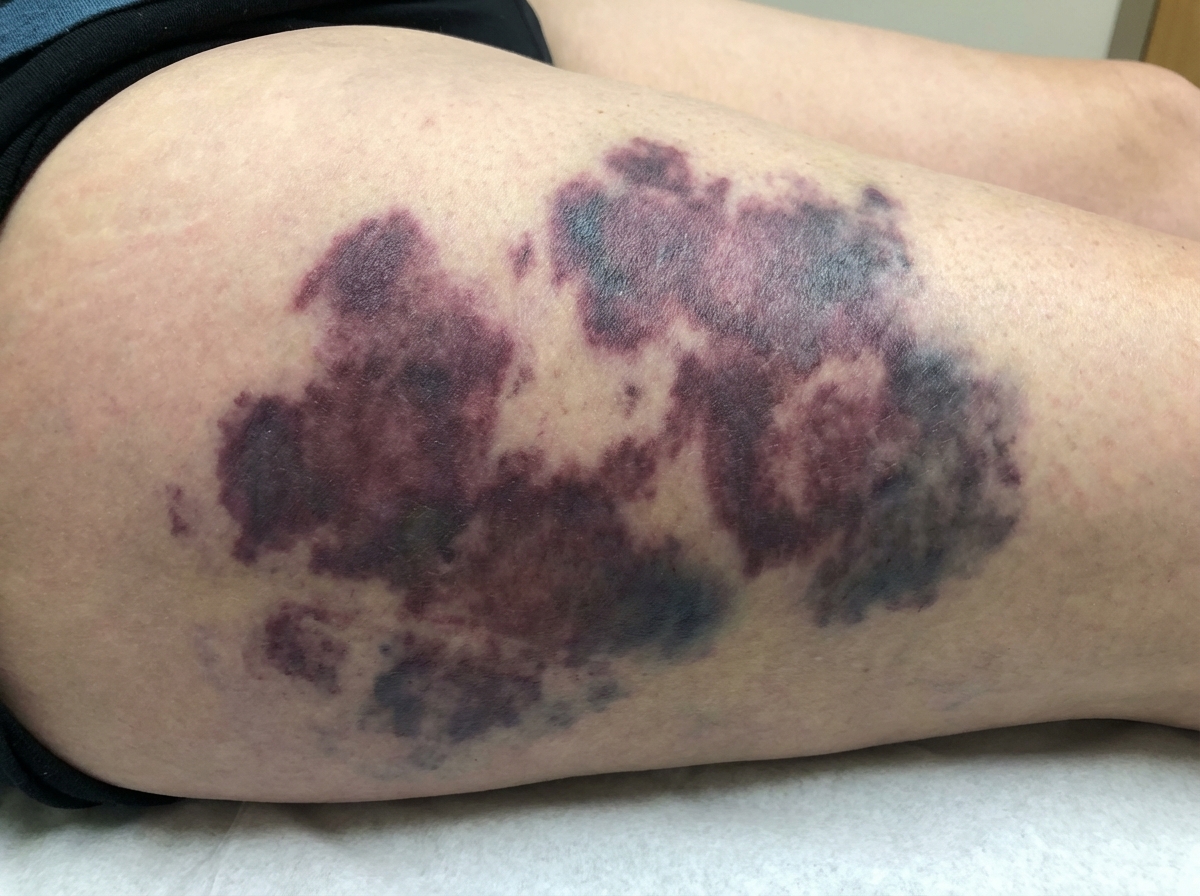
A 68-year-old man comes to the emergency department 12 hours after the appearance of tender, purple discolorations on his thighs and lower abdomen. He began taking a medication 4 days ago after failed cardioversion for atrial fibrillation, but he cannot remember the name. Physical examination shows a tender bluish-black discoloration on the anterior abdominal wall. A photograph of the right thigh is shown. Which of the following is the most likely explanation for this patient's skin findings?
A 35-year-old female presents to her primary care physician complaining of right upper quadrant pain over the last 6 months. Pain is worst after eating and feels like intermittent squeezing. She also admits to lighter colored stools and a feeling of itchiness on her skin. Physical exam demonstrates a positive Murphy's sign. The vitamin level least likely to be affected by this condition is associated with which of the following deficiency syndromes?
A 59-year-old male with a 1-year history of bilateral knee arthritis presents with epigastric pain that intensifies with meals. He has been self-medicating with aspirin, taking up to 2,000 mg per day for the past six months. Which of the following medications, if taken instead of aspirin, could have minimized his risk of experiencing this epigastric pain?
A 62-year-old man presents to his primary care provider complaining of leg pain with exertion for the past 6 months. He notices that he has bilateral calf cramping with walking. He states that it is worse in his right calf than in his left, and it goes away when he stops walking. He has also noticed that his symptoms are progressing and that this pain is occurring sooner than before. His medical history is remarkable for type 2 diabetes mellitus and 30-pack-year smoking history. His ankle-brachial index (ABI) is found to be 0.80. Which of the following can be used as initial therapy for this patient's condition?
A 26-year-old G1P0 woman is brought to the emergency room by her spouse for persistently erratic behavior. Her spouse reports that she has been sleeping > 1 hour a night, and it sometimes seems like she’s talking to herself. She has maxed out their credit cards on baby clothes. The patient’s spouse reports this has been going on for over a month. Since first seeing a physician, she has been prescribed multiple first and second generation antipsychotics, but the patient’s spouse reports that her behavior has failed to improve. Upon examination, the patient is speaking rapidly and occasionally gets up to pace the room. She reports she is doing “amazing,” and that she is “so excited for the baby to get here because I’m going to be the best mom.” She denies illicit drug use, audiovisual hallucinations, or suicidal ideation. The attending psychiatrist prescribes a class of medication the patient has not yet tried to treat the patient’s psychiatric condition. In terms of this new medication, which of the following is the patient’s newborn most likely at increased risk for?
A 27-year-old man presents to the emergency department for bizarre behavior. The patient had boarded up his house and had been refusing to leave for several weeks. The police were called when a foul odor emanated from his property prompting his neighbors to contact the authorities. Upon questioning, the patient states that he has been pursued by elves for his entire life. He states that he was tired of living in fear, so he decided to lock himself in his house. The patient is poorly kempt and has very poor dentition. The patient has a past medical history of schizophrenia which was previously well controlled with olanzapine. The patient is restarted on olanzapine and monitored over the next several days. Which of the following needs to be monitored long term in this patient?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app