
Autonomic/CV Drugs — MCQs

On this page
A 22-year-old woman comes to the physician to discuss the prescription of an oral contraceptive. She has no history of major medical illness and takes no medications. She does not smoke cigarettes. She is sexually active with her boyfriend and has been using condoms for contraception. Physical examination shows no abnormalities. She is prescribed combined levonorgestrel and ethinylestradiol tablets. Which of the following is the most important mechanism of action of this drug in the prevention of pregnancy?
A 64-year-old woman presents to the clinic with a history of 3 fractures in the past year with the last one being last month. Her bone-density screening from last year reported a T-score of -3.1 and she was diagnosed with osteoporosis. She was advised to quit smoking and was asked to adapt to a healthy lifestyle to which she complied. She was also given calcium and vitamin D supplements. After a detailed discussion with the patient, the physician decides to start her on weekly alendronate. Which of the following statements best describes this patient’s new therapy?
A 7-year-old boy presents to an urgent care clinic from his friend’s birthday party after experiencing trouble breathing. His father explains that the patient had eaten peanut butter at the party, and soon after, he developed facial flushing and began scratching his face and neck. This has never happened before but his father says that they have avoided peanuts and peanut butter in the past because they were worried about their son having an allergic reaction. The patient has no significant medical history and takes no medications. His blood pressure is 94/62 mm Hg, heart rate is 125/min, and respiratory rate is 22/min. On physical examination, his lips are edematous and he has severe audible stridor. Of the following, which type of hypersensitivity reaction is this patient experiencing?
A group of researchers is studying various inhaled substances to determine their anesthetic properties. In particular, they are trying to identify an anesthetic with fast onset and quick recovery for use in emergencies. They determine the following data: Inhalational anesthetic Blood-gas partition coefficient A 0.15 B 0.92 C 5.42 Which of the following statements is accurate with regard to these inhaled anesthetic substances?
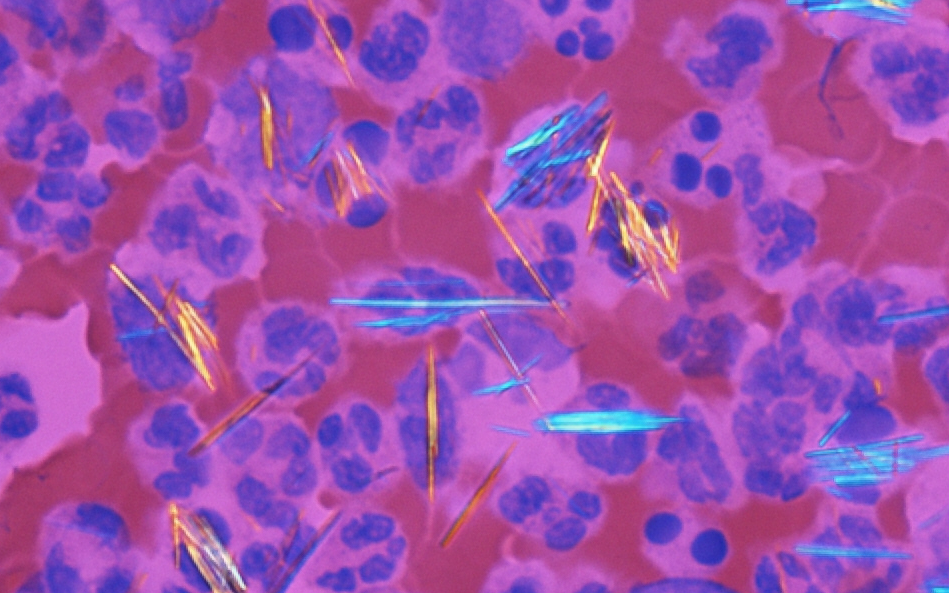
A 55-year-old man presents with intense pain in his left knee that started after returning from a camping trip 2 days ago, during which he consumed copious amounts of alcohol and red meat. He says he has had similar episodes in the past that resolved spontaneously usually over a period of about 10 days. His past medical history is significant for essential hypertension managed with hydrochlorothiazide 20 mg/day. He has a history of peptic ulcer disease and chronic kidney disease (eGFR 35 mL/min/1.73m²). The patient is afebrile, and his vital signs are within normal limits. Physical examination shows edema, warmth, and erythema of the left knee, which is also severely tender to palpation. The range of motion at the left knee joint is limited. A joint arthrocentesis of the left knee is performed, and synovial fluid analysis reveals 20,000 neutrophils and the following image is seen under polarized light microscopy (see image). Gram stain and culture of the synovial fluid show no organisms and no growth, respectively. Which of the following is the most appropriate course of treatment for this patient's condition?
A 25-year-old man comes to the physician because of an 8-hour history of painful leg cramping, runny nose, chills, diarrhea, and abdominal pain. Examination shows cool, damp skin with piloerection. The pupils are 7 mm in diameter and equal in size. Deep tendon reflexes are 3+ bilaterally. The diagnosis of opioid withdrawal is made. After the patient is stabilized, the physician initiates a withdrawal regimen with methadone. Which of the following characteristics makes this drug a suitable substance for the treatment of this patient's addiction?
An 82-year-old male with a history of congestive heart failure presented with new-onset atrial fibrillation. He was initially started on carvedilol, but he now requires an additional agent for rate control. He is started on a medicine and is warned by his physician of the following potential side effects associated with this therapy: nausea, vomiting, confusion, blurry yellow vision, electrolyte abnormalities, and potentially fatal arrhythmia. Which of the following is most likely to increase this patient's susceptibility to the toxic effects associated with this medication?
A 22-year-old woman presents to the emergency department feeling lightheaded and states that her heart is racing. She does not have a history of any chronic medical conditions. She is a college sophomore and plays club volleyball. Although she feels stressed about her upcoming final exams next week, she limits her caffeine intake to 3 cups of coffee per day to get a good night sleep. She notes that her brother takes medication for some type of heart condition, but she does not know the name of it. Both her parents are alive and well. She denies recent illness, injuries, or use of cigarettes, alcohol, or recreational drugs. The pertinent negatives from the review of systems include an absence of fever, nausea, vomiting, sweating, fatigue, or change in bowel habits. The vital signs include: temperature 36.8°C (98.2°F), heart rate 125/min, respiratory rate 15/min, blood pressure 90/75 mm Hg, and oxygen saturation of 100% on room air. The laboratory results are within normal limits. The ECG is significant for a shortened PR interval and widened QRS. Which of the following medications should the patient avoid in this scenario?
A 71-year-old man with recently diagnosed small-cell lung cancer sees his physician because of increasing weakness over the past 3 months. He is unable to climb stairs or comb his hair. His weakness is worse after inactivity and improves with exercise. He is a former smoker with a 30-pack-year history. He is currently preparing for initiation of chemotherapy. His vital signs are within normal limits. On examination, ptosis of both eyelids is seen. Dry oral mucosa is notable. Significant weakness is detected in all four proximal extremities. The patellar and biceps reflexes are absent. Auscultation of the lungs reveals generalized wheezing and rhonchi. Which of the following is the most likely underlying mechanism for this patient’s weakness?
A 50-year-old woman comes to the physician for the evaluation of excessive hair growth on her chin over the past 2 weeks. She also reports progressive enlargement of her gums. Three months ago, she underwent a liver transplantation due to Wilson disease. Following the procedure, the patient was started on transplant rejection prophylaxis. She has a history of poorly-controlled type 2 diabetes mellitus. Temperature is 37°C (98.6°F), pulse is 80/min, respirations are 22/min, and blood pressure is 150/80 mm Hg. Physical examination shows dark-pigmented, coarse hair on the chin, upper lip, and chest. The gingiva and the labial mucosa are swollen. There is a well-healed scar on her right lower abdomen. Which of the following drugs is the most likely cause of this patient's findings?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app