
Autonomic/CV Drugs — MCQs

On this page
A 56-year-old postmenopausal woman comes to the physician because of a 6-month history of worsening pain and swelling in her left knee. She has a history of peptic ulcer disease for which she takes cimetidine. Examination shows palpable crepitus and limited range of motion of the left knee. Which of the following is the most appropriate pharmacotherapy for this patient’s symptoms?
A 45-year-old man presents with a persistent cough for the past month. He says it started off with a runny nose and fever, from which he recovered in a week, but he says that the cough persists after the resolution of the fever. The patient denies any expectoration, chest pain, weight loss, or breathlessness. He reports no history of recent travel or sick contacts. Past medical history is significant for chronic constipation. He reports a 15-pack-year smoking history but denies any alcohol or current recreational drug use. He says he did use intravenous drugs in his late twenties but quit after going through a drug rehabilitation program. Physical examination is unremarkable. Laboratory findings and a chest radiograph are normal. Which of the following would be the best choice as a cough suppressant in this patient?
A 65-year-old man presents to the emergency department with shortness of breath. He was at home cleaning his yard when his symptoms began. The patient is a farmer and does not have regular medical care. He has smoked two packs of cigarettes every day for the past 40 years. The patient lives alone and admits to feeling lonely at times. His temperature is 99.5°F (37.5°C), blood pressure is 159/95 mmHg, pulse is 90/min, respirations are 19/min, and oxygen saturation is 86% on room air. On physical exam, you note a man in distress. Pulmonary exam reveals poor air movement, wheezing, and bibasilar crackles. Cardiac exam is notable for an S4 heart sound. The patient is started on appropriate therapy and his symptoms improve. Prior to discharge he is no longer distressed when breathing and his oxygen saturation is 90% on room air. Which of the following interventions could improve mortality the most in this patient?
A 24-year-old woman comes to the physician because of excessive hair growth. She has noticed increasing numbers of dark hairs on her upper lip and on her abdomen over the past 8 years. Menarche was at the age of 13 years. Menses occur at regular 28-day intervals and last 5–6 days with moderate flow. She is sexually active with one male partner. Her only medication is a combination oral contraceptive. She is 168 cm (5 ft 6 in) tall and weighs 88 kg (193 lb); BMI is 31 kg/m2. Vital signs are within normal limits. Physical examination shows coarse dark hair on the upper lip and periumbilical and periareolar skin. Her external genitalia appear normal. The remainder of the examination shows no abnormalities. Midcycle serum studies show: Fasting glucose 95 mg/dL Dehydroepiandrosterone sulfate 3.1 μg/mL (N = 0.5–5.4) Luteinizing hormone 95 mIU/mL Follicle-stimulating hormone 75 mIU/mL 17α-Hydroxyprogesterone 190 ng/dL (N = 20–300) Testosterone 1.1 nmol/L (N < 3.5) Dihydrotestosterone 435 pg/mL (N < 300) A urine pregnancy test is negative. Which of the following is the most likely underlying cause of this patient's symptom?
A 14-year-old female with no past medical history presents to the emergency department with nausea and abdominal pain. On physical examination, her blood pressure is 78/65, her respiratory rate is 30, her breath has a fruity odor, and capillary refill is > 3 seconds. Serum glucose is 820 mg/dL. After starting IV fluids, what is the next best step in the management of this patient?
A 52-year-old man comes to the physician because of increasing weakness of his arms and legs over the past year. He has also had difficulty speaking for the past 5 months. He underwent a partial gastrectomy for gastric cancer 10 years ago. His temperature is 37.1°C (98.8°F), pulse is 88/min, and blood pressure is 118/70 mm Hg. Examination shows dysarthria. There is mild atrophy and twitching of the tongue. Muscle strength is decreased in all extremities. Muscle tone is decreased in the right lower extremity and increased in the other extremities. Deep tendon reflexes are absent in the right lower extremity and 4+ in the other extremities. Plantar reflex shows an extensor response on the left. Sensation is intact in all extremities. Which of the following is the most appropriate pharmacotherapy for this patient?
A 56-year-old man with substernal chest pain calls 911. When paramedics arrive, they administer drug X sublingually for the immediate relief of angina. What is the most likely site of action of drug X?
A 78-year-old woman with a history of cerebrovascular accident (CVA) presents to the emergency department with slurred speech, diplopia and dizziness that has persisted for eight hours. Upon further questioning you find that since her CVA one year ago, she has struggled with depression and poor nutrition. Her dose of paroxetine has been recently increased. Additionally, she is on anti-seizure prophylaxis due to sequelae from her CVA. CT scan reveals an old infarct with no acute pathology. Vital signs are within normal limits. On physical exam you find the patient appears frail. She is confused and has nystagmus and an ataxic gait. What would be an appropriate next step?
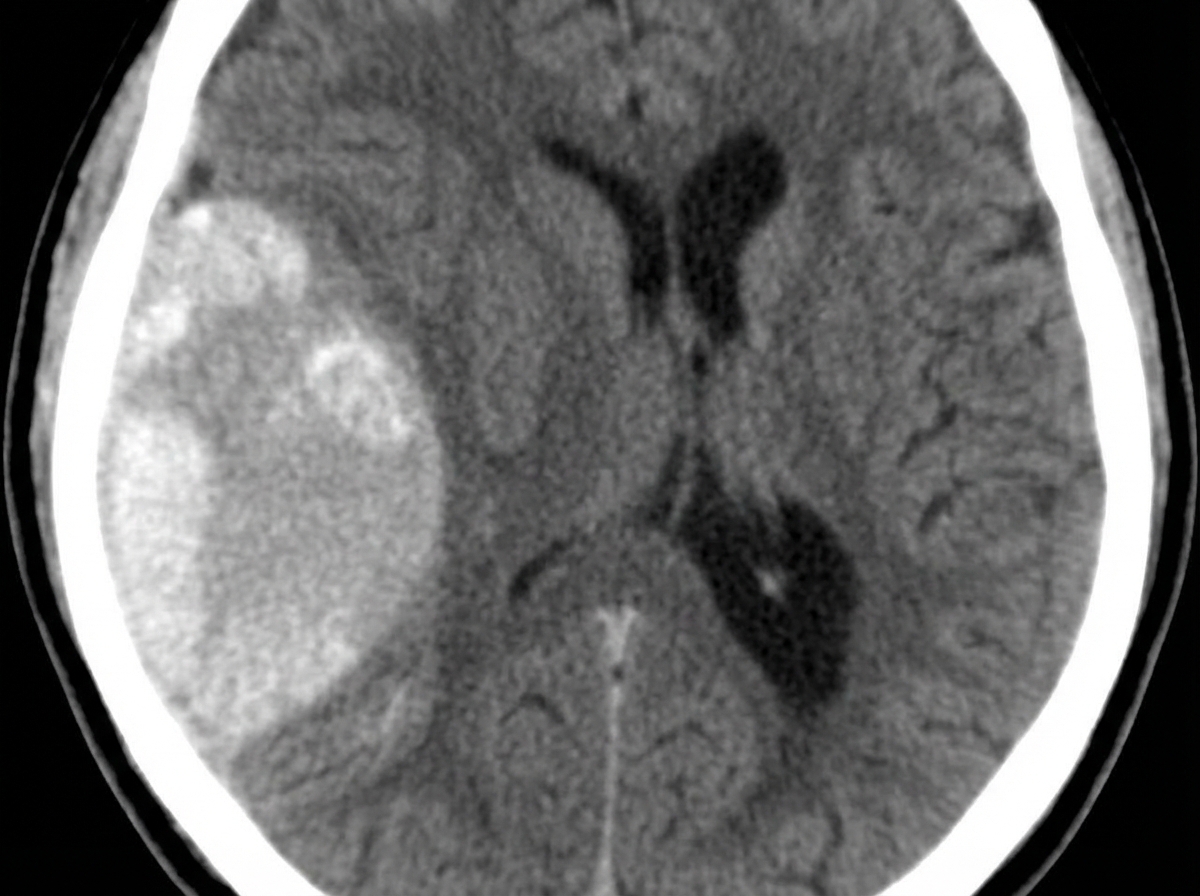
A 23-year-old man presents with a blunt force injury to the head from a baseball bat. He is currently unconscious, although his friends say he was awake and speaking with them en route to the hospital. He has no significant past medical history and takes no current medications. The vital signs include: temperature 37.0°C (98.6°F), blood pressure 165/85 mm Hg, pulse 50/min, and respiratory rate 19/min. On physical examination, there is a blunt force injury to the left temporoparietal region approximately 10.1–12.7 cm (4–5 in) in diameter. There is anisocoria of the left pupil, which is unresponsive to light. The patient is intubated and fluid resuscitation is initiated. A noncontrast computed tomography (CT) scan of the head is acquired and shown in the exhibit (see image). Which of the following is the most appropriate medical treatment for this patient?
A patient in a phase 1 trial for a novel epoxide reductase inhibitor, being studied for stroke prophylaxis, develops pain and erythema on the right thigh two days after starting the trial. This rapidly progresses to a purpuric rash with necrotic bullae within 24 hours. Lab results show a PTT of 29 seconds, PT of 28 seconds, and INR of 2.15. What is the most likely pathogenesis of this condition?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app