
Autonomic/CV Drugs — MCQs

On this page
A 36-year-old woman is brought to the emergency department because of lightheadedness, weakness, and abdominal pain for 6 hours. Over the past 3 days, she has also had severe nausea, vomiting, and watery diarrhea. She was diagnosed with pulmonary sarcoidosis 2 years ago. Current medications include prednisone. Her temperature is 38.9°C (102.0°F), pulse is 112/min, and blood pressure is 85/50 mm Hg. Physical examination shows a round face with prominent preauricular fat pads. Her fingerstick blood glucose concentration is 48 mg/dL. Further evaluation is most likely to show which of the following laboratory changes?
A 65-year-old woman presents with complaints of difficulty sleeping due to discomfort in her legs for the past 6 months. She is unable to describe the discomfort, but says it is an unpleasant, creeping and crawling feeling that is not painful. She feels an irresistible urge to move her legs to decrease the discomfort. The unpleasant sensation in her legs often occurs at night when she is lying in bed. She is recently divorced and lives alone. She denies any changes in appetite, weight loss, low mood, or suicidal thoughts. The physical examination is unremarkable except for signs of mild pallor. Laboratory test results show microcytic anemia with hemoglobin of 9.8 g/dL and decreased serum iron and ferritin levels. Apart from correcting her anemia, which additional drug would you prescribe for her symptoms?
A 42-year-old man is brought to the emergency department by police. He was found obtunded at a homeless shelter. The patient has a past medical history of alcohol abuse, intravenous (IV) drug use, schizophrenia, hepatitis C, and anxiety. His current medications include disulfiram, intramuscular haloperidol, thiamine, and clonazepam. The patient is non-compliant with his medications except for his clonazepam. His temperature is 99.5°F (37.5°C), blood pressure is 110/67 mmHg, pulse is 100/min, respirations are 16/min, and oxygen saturation is 96% on room air. On physical exam, the patient is covered in bruises, and his nose is bleeding. The patient's abdomen is distended and positive for a fluid wave. IV fluids are started, and the patient is also given thiamine, folic acid, and magnesium. It is noted by the nursing staff that the patient seems to be bleeding at his IV sites. Laboratory values are ordered and return as below: Hemoglobin: 10 g/dL Hematocrit: 25% Leukocyte count: 7,500 cells/mm^3 with normal differential Platelet count: 65,000/mm^3 Serum: Na+: 139 mEq/L Cl-: 102 mEq/L K+: 4.1 mEq/L HCO3-: 24 mEq/L BUN: 24 mg/dL Glucose: 77 mg/dL Creatinine: 1.4 mg/dL Ca2+: 9.9 mg/dL D-dimer: < 250 ng/mL AST: 79 U/L ALT: 52 U/L Which of the following is most likely to help with this patient's bleeding?
A 7-year-old boy presents with frequent episodes of blanking out or daydreaming. Each episode lasts for less than 10 seconds. During the episode, he is unaware of what is going on around him and does not respond to questions or calling his name. After the episode, he continues whatever he was doing before. An EEG is performed during one of these episodes, which shows generalized 3–4 Hz 'spike-and-dome' wave complexes. What is the mechanism of action of the drug recommended to treat this patient’s condition?
A previously healthy 9-year-old boy is brought to the physician by his mother because of a 3-month history of episodic abdominal pain. During this time, he has been more tired than usual. For the past 2 months, he has also had bulky stools that are difficult to flush. His maternal aunt has systemic lupus erythematosus. The boy is at the 31st percentile for height and 5th percentile for weight. Vital signs are within normal limits. Examination shows scattered ecchymoses across bilateral knees, the left forearm, and the upper back. The abdomen is mildly distended; bowel sounds are hyperactive. Laboratory studies show: Hemoglobin 11.1 g/dL Leukocyte count 4,500/mm3 Platelet count 243,000/mm3 Mean corpuscular volume 78 μm3 Bleeding time 5 minutes Prothrombin time 24 seconds Partial thromboplastin time 45 seconds Further evaluation is most likely to show which of the following?
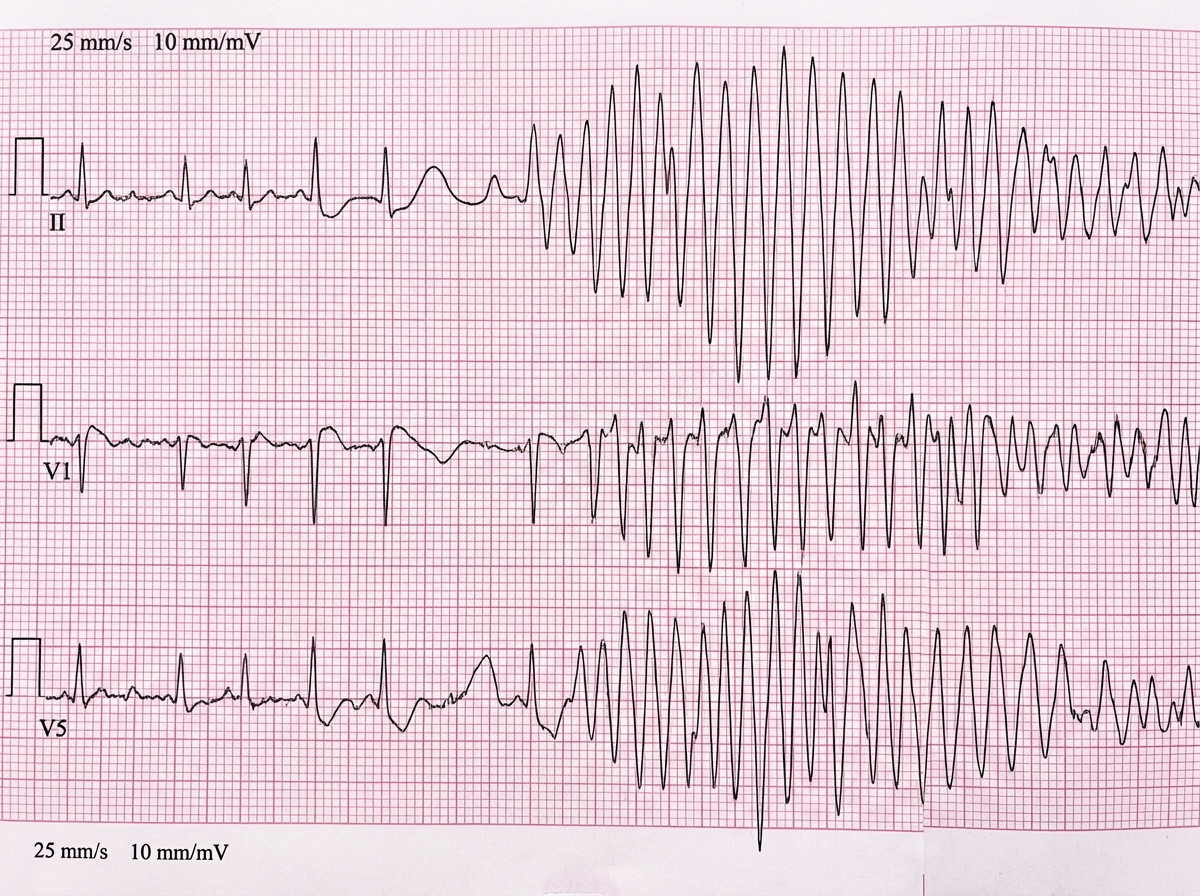
Two days after being admitted for pneumonia, a 70-year-old man has repeated episodes of palpitations and nausea. He does not feel lightheaded and does not have chest pain. The patient appears mildly distressed. His pulse is 59/min and blood pressure is 110/60 mm Hg. Examination shows no abnormalities. Sputum cultures taken at the time of admission were positive for Mycoplasma pneumoniae. His magnesium is 2.0 mEq/L and his potassium is 3.7 mEq/L. An ECG taken during an episode of palpitations is shown. Which of the following is the most appropriate next step in management?
A 58-year-old female comes to the physician because of generalized fatigue and malaise for 3 months. Four months ago, she was treated for a urinary tract infection with trimethoprim-sulfamethoxazole. She has hypertension, asthma, chronic lower back pain, and chronic headaches. Current medications include hydrochlorothiazide, an albuterol inhaler, naproxen, and an aspirin-caffeine combination. Examination shows conjunctival pallor. Laboratory studies show: Hemoglobin 8.9 g/dL Serum Urea nitrogen 46 mg/dL Creatinine 2.4 mg/dL Calcium 9.8 mg/dL Urine Protein 1+ Blood 1+ RBCs none WBCs 9-10/hpf Urine cultures are negative. Ultrasound shows shrunken kidneys with irregular contours and papillary calcifications. Which of the following is the most likely underlying mechanism of this patient's renal failure?
A 32-year-old man presents with excessive urination. He reports that he urinates 10 times a day and wakes up multiple times a night to pee. He complains that this is affecting both his social life and his ability to concentrate at work. He states that he always has an “active bladder,” but his symptoms worsened when he started meeting with a physical trainer last month who told him he should increase his water intake to prevent dehydration. The patient has a history of migraines and bipolar I disorder. His medications include metoprolol, lithium, and naproxen as needed. A basic metabolic panel is performed, and the results are shown below: Serum: Na+: 149 mEq/L Cl-: 102 mEq/L K+: 3.4 mEq/L HCO3-: 26 mEq/L Urea nitrogen: 12 mg/dL Creatinine: 1.0 mg/dL Glucose: 78 mg/dL Ca2+: 9.5 mg/dL A urinalysis is obtained, which reveals pale-colored urine with a specific gravity of 0.852 and a urine osmolarity of 135 mOsm/L. The patient undergoes a water deprivation test. The patient’s urine specific gravity increases to 0.897 and urine osmolarity is now 155 mOsm/L. The patient is given an antidiuretic hormone analogue. Urine osmolarity rises to 188 mOsm/L. Which of the following is the best initial management for the patient’s most likely condition?
An anesthesiologist is preparing a patient for a short surgical procedure. The physician would like to choose a sedating agent that can be given intravenously and will have a quick onset of action and short half-life. Which of the following agents would be ideal for this purpose?
A 57-year-old woman presents to her physician for a checkup. The past medical history is significant for diabetes mellitus type 2, and a history of myocardial infarction. The current medications are aspirin, lisinopril, metoprolol, atorvastatin, and metformin. The patient’s HbA1c is 7.9%, and her fasting blood glucose is 8.9 mmol/L (160 mg/dL). Which of the following statements regarding the use of exenatide in this patient is most correct?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app