
Autonomic/CV Drugs — MCQs

On this page
A 35-year-old woman is admitted to the medical unit for worsening renal failure. Prior to admission, she was seen by her rheumatologist for a follow-up visit and was found to have significant proteinuria and hematuria on urinalysis and an elevated serum creatinine. She reports feeling ill and has noticed blood in her urine. She was diagnosed with systemic lupus erythematosus at the age of 22, and she is currently being treated with ibuprofen for joint pain and prednisone for acute flare-ups. Her blood pressure is 165/105 mmHg. Laboratory testing is remarkable for hypocomplementemia and an elevated anti-DNA antibody. A renal biopsy is performed, which demonstrates 65% glomerular involvement along with the affected glomeruli demonstrating endocapillary and extracapillary glomerulonephritis. In addition to glucocorticoid therapy, the medical team will add mycophenolate mofetil to her treatment regimen. Which of the following is the mechanism of action of mycophenolate mofetil?
A 65-year-old woman is transferred to the intensive care unit after she underwent coronary stenting for a posterior-inferior STEMI. She is known to have allergies to amiodarone and captopril. A few hours after the transfer, she suddenly loses consciousness. The monitor shows ventricular fibrillation. CPR is initiated. After 3 consecutive shocks with a defibrillator, the monitor shows ventricular fibrillation. Which of the following medications should be administered next?
A 62-year-old man presents to his geriatrician due to waking several times during the night and also rising too early in the morning. He says this has worsened over the past 7 months. In the morning, he feels unrefreshed and tired. His medical history is positive for hypertension and benign prostatic hyperplasia. He has never been a smoker. He denies drinking alcohol or caffeine prior to bedtime. Vital signs reveal a temperature of 36.6°C (97.8°F), blood pressure of 130/80 mm Hg, and heart rate of 77/min. Physical examination is unremarkable. After discussing good sleep hygiene with the patient, which of the following is the best next step in the management of this patient’s condition?
An ECG from an 8-year-old male with neurosensory deafness and a family history of sudden cardiac arrest demonstrates QT-interval prolongation. Which of the following is this patient most at risk of developing?
A 72-year-old man is brought to the emergency department from hospice. The patient has been complaining of worsening pain over the past few days and states that it is no longer bearable. The patient has a past medical history of pancreatic cancer which is being managed in hospice. The patient desires no "heroic measures" to be made with regards to treatment and resuscitation. His temperature is 98.8°F (37.1°C), blood pressure is 107/68 mmHg, pulse is 102/min, respirations are 22/min, and oxygen saturation is 99% on room air. Physical exam reveals an uncomfortable elderly man who experiences severe pain upon abdominal palpation. Laboratory values reveal signs of renal failure, liver failure, and anemia. Which of the following is the best next step in management?
A 58-year-old woman comes to the physician for evaluation of vaginal dryness and pain during sexual intercourse with her husband. Four months ago, she was diagnosed with metastatic breast cancer and is currently undergoing chemotherapy. She has smoked one pack of cigarettes daily for 15 years but quit when she was diagnosed with breast cancer. Physical examination shows thinning of the vaginal mucosa. A dual-energy x-ray absorptiometry (DXA) study of her hip shows a T-score of -2.6. Six months ago, her T-score was -1.6. Which of the following drugs is most likely exacerbating this patient's symptoms?
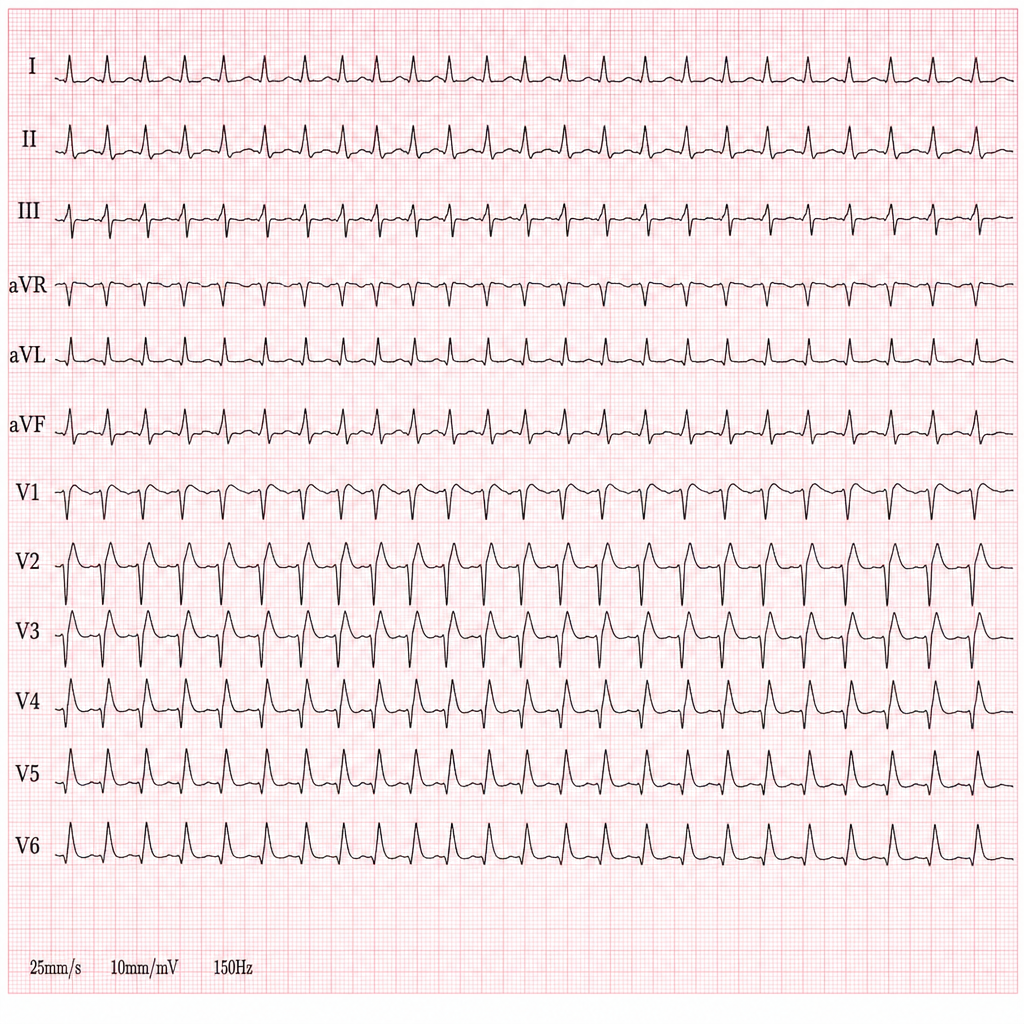
A 44-year-old woman presents with palpitations and lightheadedness. She says that symptoms onset 3 days ago and have not improved. She denies any similar episodes in this past. Her blood pressure is 140/90 mm Hg, heart rate is 150/min, respiratory rate is 16/min, and temperature is 36.6℃ (97.9℉). An ECG is performed and the results are shown in the picture. For cardioversion, it is decided to use an antiarrhythmic agent which has a use-dependent effect. Which of the following medications was most probably used?
A 26-year-old G1P0 presents to her first obstetric visit after having a positive urine pregnancy test at home. Her last menstrual period was 9 weeks ago. She has no past medical history, but her mother has rheumatoid arthritis. The patient states that for several weeks, she has felt especially warm, even when her co-workers do not, and had muscle weakness. She also complains of mood swings and fatigue. At this visit, her temperature is 99.0°F (37.2°C), blood pressure is 140/81 mmHg, pulse is 106/min, and respirations are 17/min. Physical exam is notable for 3+ deep tendon reflexes bilaterally and 4/5 strength in both hips and shoulders. Ultrasound confirms the presence of a heart beat and shows a crown rump length that is consistent with a gestational age of 9 weeks and 3 days. Which of the following is the best therapy for this patient?
A 69-year-old man is brought to the emergency room by his daughter due to confusion. She reports that her father did not remember who she was yesterday, and his refrigerator was completely empty when she tried to make him lunch. She states that he was acting like himself when she visited him last week. She also notes that he has struggled with alcoholism for many years and has not seen a doctor in over two decades. She is unsure if he has any other chronic medical conditions. In the emergency room, the patient’s temperature is 101.2°F (38.4°C), pulse is 103/min, respirations are 22/min, and O2 saturation is 92% on room air. His BMI is 17.1 kg/m^2. Physical exam reveals an extremely thin and frail man who is not oriented to person, place, or time. As he is being examined, he becomes unresponsive and desaturates to 84%. He is intubated and admitted to the intensive care unit for what is found to be pneumonia, and the patient is started on total parental nutrition as he is sedated and has a history of aspiration from a prior hospitalization. Two days later, physical exam is notable for new peripheral edema. Laboratory tests at that time reveal the following: Serum: Na+: 133 mEq/L Cl-: 101 mEq/L K+: 2.4 mEq/L HCO3-: 24 mEq/L BUN: 22 mg/dL Glucose: 124 mg/dL Creatinine: 1.1 mg/dL Phosphate: 1.1 mg/dL Mg2+: 1.0 mg/dL Which of the following could have prevented the complication seen in this patient?
A 60-year-old patient is at his physician’s office for a routine health maintenance exam. The patient has a past medical history of osteoarthritis in his right knee and GERD that is well-controlled with over the counter medication. On a fasting lipid profile, he is found to have high cholesterol. The patient is started on daily atorvastatin to reduce his risk of cardiovascular disease. What is the major apolipoprotein found on the lipoprotein most directly affected by his statin medication?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app