
Autonomic/CV Drugs — MCQs

On this page
A 47-year-old man with bipolar I disorder and hypertension comes to the physician because of a 2-week history of increased thirst, urinary frequency, and sleep disturbance. He says that he now drinks up to 30 cups of water daily. He has smoked 2 packs of cigarettes daily for the past 20 years. Examination shows decreased skin turgor. Serum studies show a sodium concentration of 149 mEq/L, a potassium concentration of 4.1 mEq/L, and an elevated antidiuretic hormone concentration. His urine osmolality is 121 mOsm/kg H2O. Which of the following is the most likely explanation for these findings?
A newborn infant comes to the attention of the neonatal care unit because he started having heavy and rapid breathing. In addition, he was found to be very irritable with pale skin and profuse sweating. Finally, he was found to have cold feet with diminished lower extremity pulses. Cardiac auscultation reveals a harsh systolic murmur along the left sternal border. Notably, the patient is not observed to have cyanosis. Which of the following treatments would most likely be effective for this patient's condition?
A 20-year-old man presents to your office with dyspnea, reporting nocturnal cough. You note expiratory wheezing on auscultation. Chest x-ray reveals increased anteroposterior diameter. Past medical history is significant for multiple episodes of "bronchitis" as a child. Which of the following drugs would be most effective for long-term treatment of this patient?
Forty minutes after undergoing nasal polypectomy for refractory rhinitis, a 48-year-old woman develops chest tightness and shortness of breath. The surgical course was uncomplicated and the patient was successfully extubated. She received ketorolac for postoperative pain. She has a history of asthma, hypertension, and aspirin allergy. Her daily medications include metoprolol and lisinopril. Examination shows a flushed face. Chest auscultation reveals wheezes and decreased breath sounds in both lung fields. An ECG shows no abnormalities. Which of the following is the most likely underlying cause of this patient's symptoms?
A 34-year-old male with a previous diagnosis of Grave's disease presents for a check-up. Since his diagnosis 4 months ago, the patient's symptoms have been relatively well-controlled with medications since starting them 3 weeks ago after an initial unsuccessful course of radioiodine ablation. The patient's complete blood count reveals decreased absolute neutrophils at 450/mL and a slightly decreased hematocrit of 39%. Which of the following is the most likely cause of this patient's abnormal laboratory results?
A 60-year-old male presents to the emergency room with shortness of breath after waking up in the middle of the night with a "choking" sensation. The patient has a history of hypertension and MI. Physical examination reveals bibasilar inspiratory crackles and an S3 heart sound. Which of the following drugs should be administered for rapid, significant relief of this patient's symptoms?
A 31-year-old woman makes an appointment with a fertility specialist because she has not been able to conceive despite trying for over a year with her husband. She is concerned because her husband has 2 children from a previous marriage whereas she has no children. After obtaining a detailed history as well as lab tests, the specialist prescribes a certain drug. Interestingly, this drug is able to stimulate receptors in the presence of low hormone levels and inhibit the same receptors in the presence of high hormone levels. The drug that is most likely being prescribed in this case is associated with which of the following adverse events?
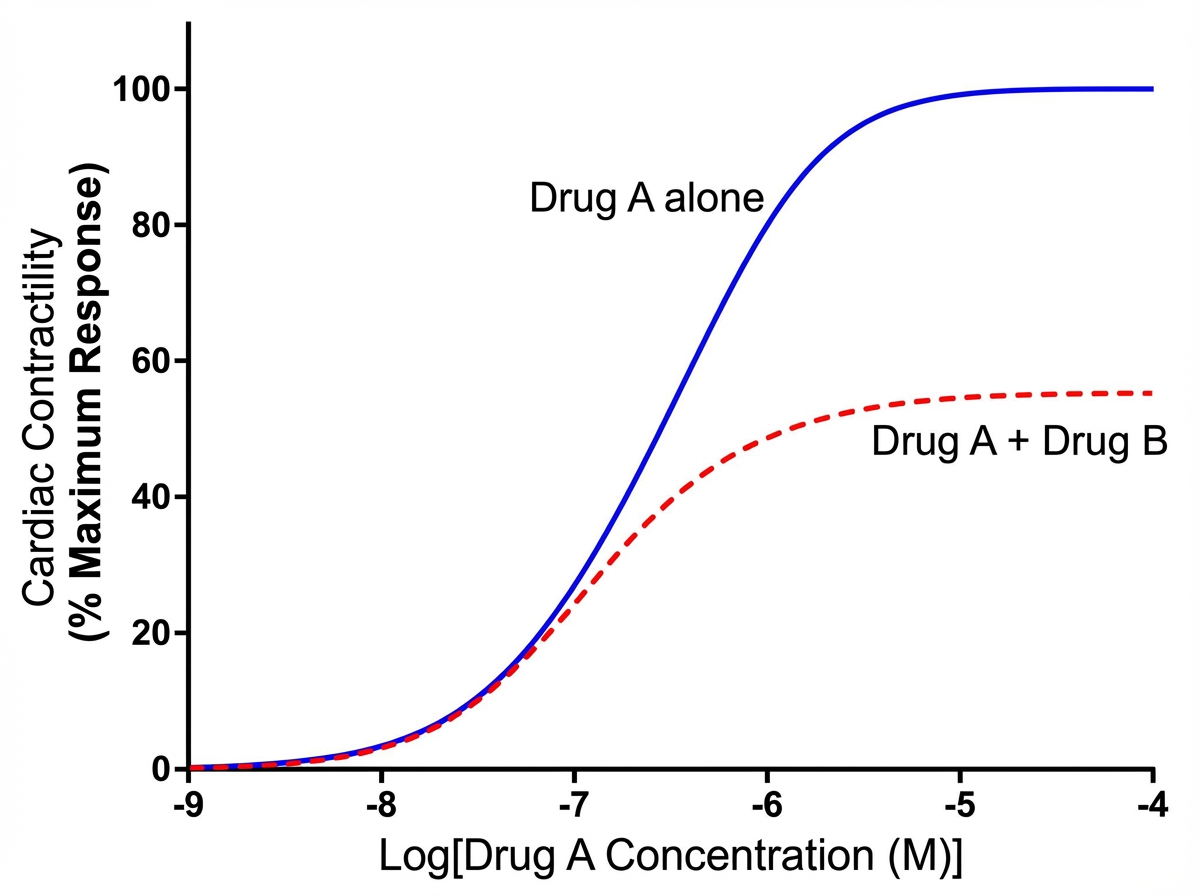
An investigator is studying the effects of different drugs on the contraction of cardiomyocytes. The myocytes are able to achieve maximal contractility with the administration of drug A, a full beta-adrenergic agonist. The subsequent administration of drug B produces the response depicted in the graph shown. Which of the following drugs is most likely to produce a response similar to that of drug B?
An 82-year-old male with congestive heart failure experiences rapid decompensation of his condition, manifesting as worsening dyspnea, edema, and increased fatigue. Labs reveal an increase in his serum creatinine from baseline. As part of the management of this acute change, the patient is given IV dobutamine to alleviate his symptoms. Which of the following effects occur as a result of this therapy?
A 52-year-old man comes to the physician because of a 3-day history of intermittent chest tightness that worsens with exercise. He has chronic atrial fibrillation treated with a drug that prolongs the QT interval. During cardiac stress testing, an ECG shows progressive shortening of the QT interval as the heart rate increases. Which of the following drugs is this patient most likely taking?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app