
Autonomic/CV Drugs — MCQs

On this page
A 44-year-old woman comes to the physician because of a 6-month history of fatigue, constipation, and a 7-kg (15.4-lb) weight gain. Menses occur irregularly in intervals of 40–50 days. Her pulse is 51/min, and blood pressure is 145/86 mm Hg. Examination shows conjunctival pallor and cool, dry skin. There is mild, nonpitting periorbital edema. Serum thyroid-stimulating hormone concentration is 8.1 μU/mL. Treatment with the appropriate pharmacotherapy is initiated. After several weeks of therapy with this drug, which of the following hormonal changes is expected?
A 50-year-old woman presents to the clinic with joint pain that has persisted for the last 2 months. She reports having intermittently swollen, painful hands bilaterally. She adds that when she wakes up in the morning, her hands are stiff and do not loosen up until an hour later. The pain tends to improve with movement. Physical examination is significant for warm, swollen, tender proximal interphalangeal joints, metacarpophalangeal joints, and wrists bilaterally. Laboratory results are positive for rheumatoid factor (4-fold greater than the upper limit of normal (ULN)) and anti-cyclic citrullinated peptide (anti-CCP) antibodies (3-fold greater than ULN). CRP and ESR are elevated. Plain X-rays of the hand joints show periarticular osteopenia and bony erosions. She was started on the first-line drug for her condition which inhibits dihydrofolate reductase. Which medication was this patient started on?
A 78-year-old woman presents to the orthopedic department for an elective total left knee arthroplasty. She has had essential hypertension for 25 years and type 2 diabetes mellitus for 35 years. She has smoked 20–30 cigarettes per day for the past 40 years. The operation was uncomplicated. On day 3 post-surgery, she complains of left leg pain and swelling. On examination, her left leg appears red and edematous, and there are dilated superficial veins on the left foot. Using Wells’ criteria, the patient is diagnosed with a provoked deep venous thrombosis. Which of the following is the best initial therapy for this patient?
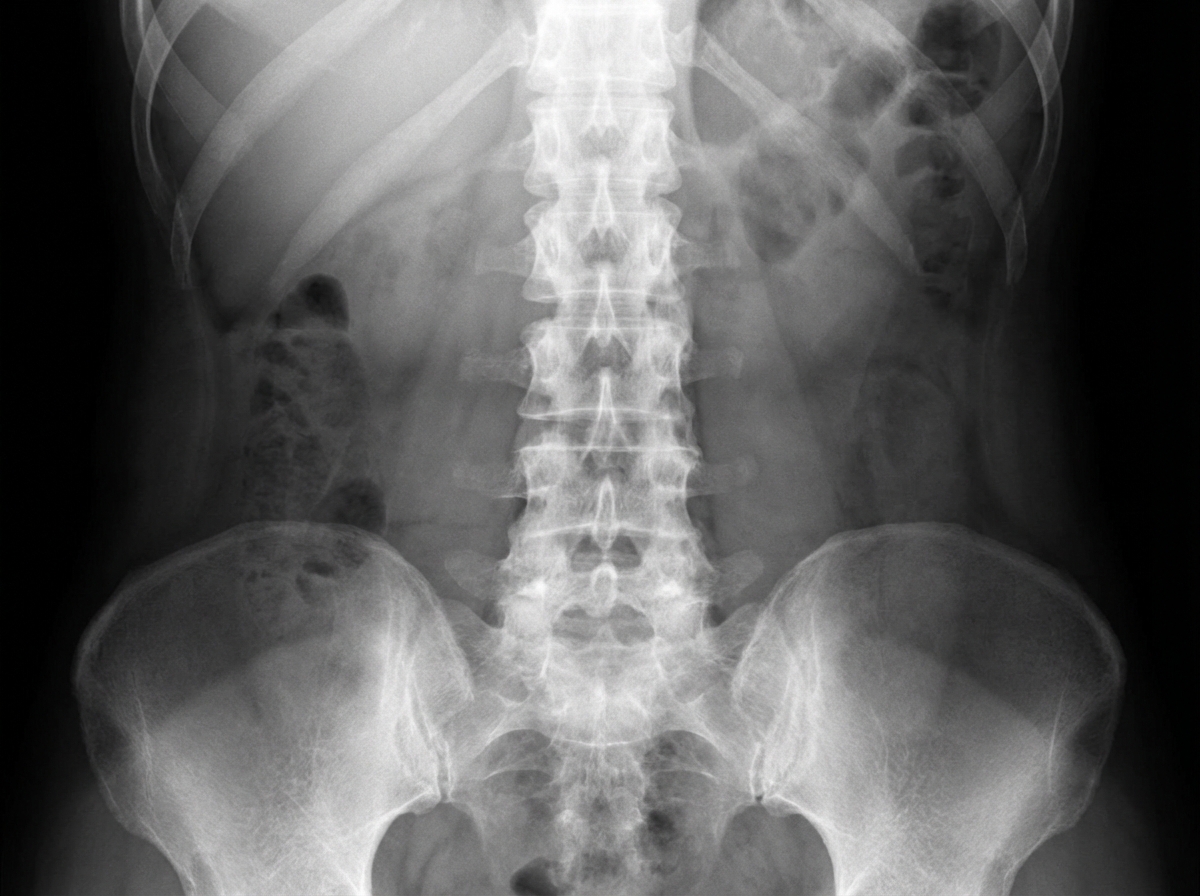
A 36-year-old man comes to the physician because of increasing back pain for the past 6 months. The pain is worse when he wakes up and improves throughout the day. He has problems bending forward. He has taken ibuprofen which resulted in limited relief. His only medication is a topical corticosteroid for two erythematous, itchy patches of the skin. His mother has rheumatoid arthritis. His temperature is 37.1°C (98.8°F), pulse is 75/min, respirations are 14/min, and blood pressure is 126/82 mmHg. Examination shows a limited spinal flexion. He has two patches with erythematous papules on his right forearm. He has tenderness on percussion of his sacroiliac joints. An x-ray of his spine is shown. Which of the following is most likely to improve mobility in this patient?
A previously healthy 46-year-old woman comes to the physician because of a 3-month history of fatigue and progressive shortness of breath. She does not take any medications. Her pulse is 93/min and blood pressure is 112/80 mm Hg. Examination shows no abnormalities. Her hemoglobin concentration is 8 g/dL, leukocyte count is 22,000/mm3, and platelet count is 80,000/mm3. A peripheral blood smear shows increased numbers of circulating myeloblasts. Bone marrow biopsy confirms the diagnosis of acute myeloid leukemia. ECG, x-ray of the chest, and echocardiogram show no abnormalities. The patient is scheduled to start induction chemotherapy with cytarabine and daunorubicin. This patient is at increased risk for which of the following long-term complications?
A 23-year-old man presents with fatigue and increased daytime somnolence. He says his symptoms began gradually 6 months ago and have progressively worsened and have begun to interfere with his job as a computer programmer. He is also bothered by episodes of paralysis upon waking from naps and reports visual hallucinations when falling asleep at night. He has been under the care of another physician for the past several months, who prescribed him the standard pharmacotherapy for his most likely diagnosis. However, he has continued to experience an incomplete remission of symptoms and has been advised against increasing the dose of his current medication because of an increased risk of adverse effects. Which of the following side effects is most closely associated with the standard drug treatment for this patient’s most likely diagnosis?
A pharmaceutical company is studying a new drug that inhibits the glucose transporter used by intestinal enterocytes to absorb glucose into the body. The drug was designed such that it would act upon the glucose transporter similarly to how cyanide acts upon cytochrome proteins. During pre-clinical studies, the behavior of this drug on the activity of the glucose transporter is examined. Specifically, enterocyte cells are treated with the drug and then glucose is added to the solution at a concentration that saturates the activity of the transporter. The transport velocity and affinity of the transporters under these conditions are then measured. Compared to the untreated state, which of the following changes would most likely be seen in these transporters after treatment?
A 65-year-old man is brought to the emergency department from his home. He is unresponsive. His son requested a wellness check because he had not heard from his father in 2 weeks. He reports that his father was sounding depressed during a telephone call. The paramedics found a suicide note and a half-empty bottle of antifreeze near the patient. The medical history includes hypertension and hyperlipidemia. The vital signs include: blood pressure 120/80 mm Hg, respiratory rate 25/min, heart rate 95/min, and temperature 37.0°C (98.5°F). He is admitted to the hospital. What do you expect the blood gas analysis to show?
A 24-year-old man presents to the postoperative unit after undergoing an appendectomy following 2 episodes of acute appendicitis. He complains of nausea and vomiting. On physical examination, his temperature is 36.9°C (98.4ºF), pulse rate is 96/minute, blood pressure is 122/80 mm Hg, and respiratory rate is 14/minute. His abdomen is soft on palpation, and bowel sounds are normoactive. Intravenous ondansetron is administered, and the patient reports relief from his symptoms. Which of the following best explains the mechanism of action of this drug?
A 57-year-old man presents for a regular check-up. He does not have any complaints at the time of presentation. He has a history of several episodes of acute non-necrotizing pancreatitis with the last episode being 2 years ago. Also, he was diagnosed with hypertension 5 years ago. Currently, he takes aspirin, atorvastatin, enalapril, and indapamide. He plays tennis twice a week, does low impact cardio workouts 3 times a week, and follows a low-fat diet. He smokes half a pack of cigarettes per day and refuses to quit smoking. The patient’s blood pressure is 140/85 mm Hg, heart rate is 88/min, respiratory rate is 14/min, and temperature is 36.6°C (97.9°F). His height is 181 cm (5 ft 11 in), weight is 99 kg (218 lb), and BMI is 30.8 kg/m2. Physical examination reveals multiple xanthomas on the patient’s trunk, elbows, and knees. Heart sounds are diminished with fixed splitting of S2 and an increased aortic component. The rest of the examination is unremarkable. The patient’s lipid profile shows the following results: Total serum cholesterol 235.9 mg/dL HDL 46.4 mg/dL LDL 166.3 mg/dL Triglycerides 600 mg/dL Glucose 99 mg/dL Which of the following modifications should be made to the patient’s therapy?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app