
Autonomic/CV Drugs — MCQs

On this page
A 56-year-old woman with rheumatoid arthritis comes to the physician for a follow-up examination. She has no other history of serious illness. Menopause occurred 1 year ago. Current medications include antirheumatic drugs and hormone replacement therapy. She exercises regularly. A DEXA scan shows a T-score of -1.80, indicating decreased bone density. Which of the following drugs is most likely involved in the pathogenesis of this finding?
Serum studies show a troponin T concentration of 6.73 ng/mL (N < 0.01), and fingerstick blood glucose concentration of 145 mg/dL. The cardiac catheterization team is activated. Treatment with unfractionated heparin, aspirin, ticagrelor, and sublingual nitroglycerin is begun, and the patient's pain subsides. His temperature is 37.3°C (99.1°F), pulse is 65/min, respirations are 23/min, and blood pressure is 91/60 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 96%. Which of the following is the most appropriate additional pharmacotherapy?
A 28-year-old female presents to her primary care provider for headache. The patient reports that every few weeks she has an episode of right-sided, throbbing headache. The episodes began several years ago and are accompanied by nausea and bright spots in her vision. The headache usually subsides if she lies still in a dark, quiet room for several hours. The patient denies any weakness, numbness, or tingling during these episodes. Her past medical history is significant for acne, hypothyroidism, obesity, and endometriosis. Her home medications include levothyroxine, oral contraceptive pills, and topical tretinoin. She has two glasses of wine with dinner several nights a week and has never smoked. She works as a receptionist at a marketing company. On physical exam, the patient has no focal neurologic deficits. A CT of the head is performed and shows no acute abnormalities. Which of the following is the most appropriate treatment for this patient during these episodes?
A 55-year-old man with a history of congestive heart failure, hypertension, and hyperlipidemia presents to his primary care clinic. He admits he did not adhere to a low salt diet on a recent vacation. He now has progressive leg swelling and needs two pillows to sleep because he gets short of breath when lying flat. Current medications include aspirin, metoprolol, lisinopril, atorvastatin, and furosemide. His physician decides to increase the dosage and frequency of the patient’s furosemide. Which of the following electrolyte abnormalities is associated with loop diuretics?
A 45-year-old woman comes to the emergency department with recurrent episodes of shaking, sweating, and palpitations. The patient is confused and complains of hunger. One week ago, she had similar symptoms that improved after eating. She has hypertension and a history of biliary pancreatitis. She underwent cholecystectomy 1 year ago. She works as a nurse aide in a nursing care facility. She does not smoke or drink alcohol. She does not exercise. Her temperature is 36.7°C (98°F), pulse is 104/min, respirations are 20/min, and blood pressure is 135/88 mm Hg. Examination shows tremors and diaphoresis. Laboratory studies show: Blood glucose 50 mg/dL Thyroid-stimulating hormone 1 mU/L C-peptide 0.50 ng/mL (N=0.8–3.1) Abdominal ultrasound reveals a 1-cm anechoic lesion in the head of the pancreas. Which of the following is the most likely cause of this patient's symptoms?
A 76-year-old woman comes to the physician because of a sudden loss of vision in her right eye for 10 minutes that morning, which subsided spontaneously. Over the past 2 months, she has had multiple episodes of left-sided headaches and pain in her jaw while chewing. Examination shows conjunctival pallor. Range of motion of the shoulders and hips is slightly limited by pain. Her erythrocyte sedimentation rate is 69 mm/h. Treatment with the appropriate medication for this patient's condition is initiated. Which of the following sets of laboratory findings is most likely as a consequence of treatment? | Lymphocytes | Neutrophils | Eosinophils | Fibroblasts |
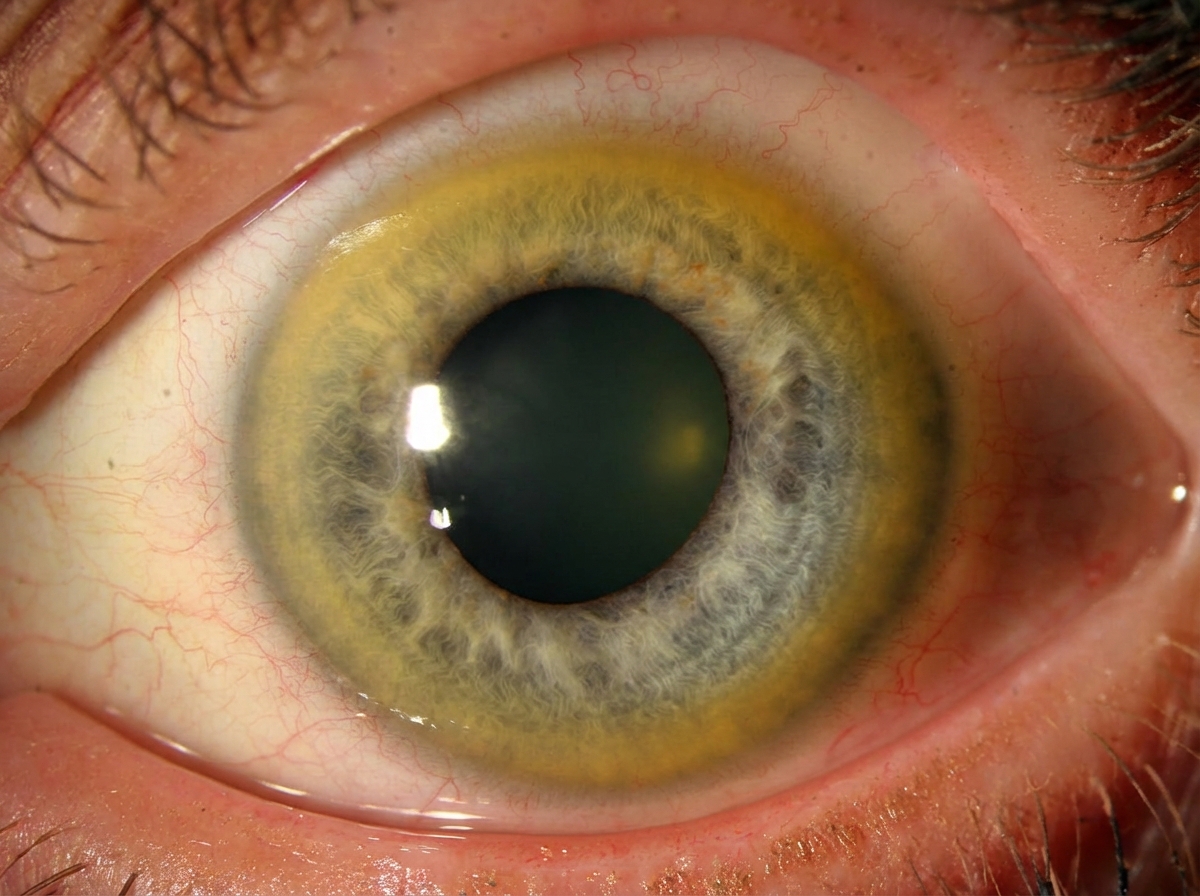
A 23-year-old man comes to the physician because of a tremor in his right hand for the past 3 months. The tremor has increased in intensity and he is unable to perform his daily activities. When he wakes up in the morning, his pillow is soaked in saliva. During this period, he has been unable to concentrate in his college classes. He has had several falls over the past month. He has no past history of serious illness. He appears healthy. His vital signs are within normal limits. Examination shows a broad-based gait. There is a low frequency tremor that affects the patient's right hand to a greater extent than his left. When the patient holds his arms fully abducted with his elbows flexed, he has a bilateral low frequency arm tremor that increases in amplitude the longer he holds his arms up. Muscle strength is normal in all extremities. Sensation is intact. Deep tendon reflexes are 4+ bilaterally. Dysmetria is present. A photograph of the patient's eye is shown. Mental status examination shows a restricted affect. The rate and rhythm of his speech is normal. Which of the following is the most appropriate pharmacotherapy?
A previously healthy 61-year-old man comes to the physician because of bilateral knee pain for the past year. The pain is worse with movement and is relieved with rest. Physical examination shows crepitus, pain, and decreased range of motion with complete flexion and extension of both knees. There is no warmth, redness, or swelling. X-rays of both knees show irregular joint space narrowing, osteophytes, and subchondral cysts. Which of the following is the most appropriate pharmacotherapy?
A 72-year-old man with congestive heart failure is brought to the emergency department because of chest pain, shortness of breath, dizziness, and palpitations for 30 minutes. An ECG shows a wide complex tachycardia with a P-wave rate of 105/min, an R-wave rate of 130/min, and no apparent relation between the two. Intravenous pharmacotherapy is initiated with a drug that prolongs the QRS and QT intervals. The patient was most likely treated with which of the following drugs?
You are a resident on an anesthesiology service and are considering using nitrous oxide to assist in placing a laryngeal mask airway (LMA) in your patient, who is about to undergo a minor surgical procedure. You remember that nitrous oxide has a very high minimal alveolar concentration (MAC) compared to other anesthetics. This means that nitrous oxide has:
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app