
Autonomic/CV Drugs — MCQs

On this page
A 36-year-old man comes to the clinic for follow-up of his general anxiety disorder. He was diagnosed a year ago for excessive worry and irritability and was subsequently started on paroxetine. He demonstrated great response to therapy but is now complaining of decreased libido, which is affecting his marriage and quality of life. He wishes to switch to a different medication at this time. Following a scheduled tapering of paroxetine, the patient is started on a different medication that is a partial agonist of the 5-HT1A receptor. Which of the following is the most likely drug that was prescribed?
A 28-year-old woman presents with weakness, fatigability, headache, and faintness. She began to develop these symptoms 4 months ago, and their intensity has been increasing since then. Her medical history is significant for epilepsy diagnosed 4 years ago. She was prescribed valproic acid, which, even at a maximum dose, did not control her seizures. She was prescribed phenytoin 6 months ago. Currently, she takes 300 mg of phenytoin sodium daily and is seizure-free. She also takes 40 mg of omeprazole daily for gastroesophageal disease, which was diagnosed 4 months ago. She became a vegan 2 months ago. She does not smoke and consumes alcohol occasionally. Her blood pressure is 105/80 mm Hg, heart rate is 98/min, respiratory rate is 14/min, and temperature is 36.8℃ (98.2℉). Her physical examination is significant only for paleness. Blood test shows the following findings: Erythrocytes 2.5 x 109/mm3 Hb 9.7 g/dL Hct 35% Mean corpuscular hemoglobin 49.9 pg/cell (3.1 fmol/cell) Mean corpuscular volume 136 µm3 (136 fL) Reticulocyte count 0.1% Total leukocyte count 3110/mm3 Neutrophils 52% Lymphocytes 37% Eosinophils 3% Monocytes 8% Basophils 0% Platelet count 203,000/mm3 Which of the following factors most likely caused this patient’s condition?
A 40-year-old man presents with multiple episodes of sudden-onset severe pain in his right side of the face lasting for only a few seconds. He describes the pain as lancinating, giving the sensation of an electrical shock. He says the episodes are precipitated by chewing or touching the face. Which of the following side effects is characteristic of the drug recommended for treatment of this patient’s most likely condition?
A 14-year-old boy comes to the physician for a follow-up after a blood test showed a serum triglyceride level of 821 mg/dL. Several of his family members have familial hypertriglyceridemia. The patient is prescribed a fibrate medication that increases his risk of gallstone disease. The expected beneficial effect of this drug is most likely due to which of the following actions?
A 29-year-old woman came to the emergency department due to severe symptoms of intoxication and unexplained convulsions. She is accompanied by her husband who reports that she takes disulfiram. There is no prior personal and family history of epilepsy. She shows signs of confusion, hyperirritability, and disorientation. On further evaluation, the patient is noted to have stomatitis, glossitis, and cheilosis. A chest X-ray is unremarkable. The deficiency of which of the vitamins below is likely to be the major cause of this patient’s symptoms?
A 4-month-old girl with Down syndrome is brought into the pediatrician’s office by her father for her first well-child visit. The father states she was a home birth at 39 weeks gestation after an uneventful pregnancy without prenatal care. The child has not received any routine immunizations. The father states that sometimes when she is crying or nursing she "gets a little blue", but otherwise the patient is healthy. The patient is within the normal range of weight and height. Her blood pressure is 110/45 mm Hg, the pulse is 185/min, the respiratory rate is 25/min, and the temperature is 37.1°C (98.7°F). The physician notes an elevated heart rate, widened pulse pressure, and some difficulty breathing. On exam, the patient is playful and in no apparent distress. On lung exam, some faint crackles are heard at the lung bases without wheezing. Cardiac exam is significant for a harsh, machine-like murmur. An echocardiogram verifies the diagnosis. What is the next step in treatment of this patient?
A 70-year-old man presents to an urgent care clinic with bilateral flank pain for the past 2 days. During the last week, he has been experiencing some difficulty with urination, which prevented him from leaving his home. Now, he has to go to the bathroom 4–5 times per hour and he wakes up multiple times during the night to urinate. He also complains of straining and difficulty initiating urination with a poor urinary stream. The temperature is 37.5°C (99.5°F), the blood pressure is 125/90 mm Hg, the pulse is 90/min, and the respiratory rate is 18/min. The physical examination showed bilateral flank tenderness and palpable kidneys bilaterally. A digital rectal exam revealed a smooth, severely enlarged prostate without nodules. A CT scan is obtained. He is prescribed a drug that will alleviate his symptoms by reducing the size of the prostate. Which of the following best describes the mechanism of action of this drug?
A 23-year-old woman presents with flatulence and abdominal cramping after meals. For the last year, she has been feeling uneasy after meals and sometimes has severe pain after eating breakfast in the morning. She also experiences flatulence and, on rare occasions, diarrhea. She says she has either cereal or oats in the morning which she usually consumes with a glass of milk. The patient is afebrile and vital signs are within normal limits. Physical examination is unremarkable. Which of the following drugs should be avoided in this patient?
A 60-year-old man visits his primary care doctor after being discharged from the hospital 3 weeks ago. He presented to the hospital with chest pain and was found to have ST elevations in leads I, aVL, and V6. He underwent cardiac catheterization with balloon angioplasty and was discharged on appropriate medications. At this visit, he complains of feeling deconditioned over the past week. He states that he is not able to jog his usual 3 miles and feels exhausted after walking up stairs. He denies chest pain. His temperature is 98.6°F (37°C), blood pressure is 101/62 mmHg, pulse is 59/min, and respirations are 18/min. His cardiac exam is notable for a 2/6 early systolic murmur at the left upper sternal border. He describes mild discomfort with palpation of his epigastrium. The remainder of his exam is unremarkable. His laboratory workup is shown below: Hemoglobin: 8 g/dL Hematocrit: 25 % Leukocyte count: 11,000/mm^3 with normal differential Platelet count: 400,000/mm^3 Serum: Na+: 136 mEq/L Cl-: 103 mEq/L K+: 3.8 mEq/L HCO3-: 25 mEq/L BUN: 45 mg/dL Glucose: 89 mg/dL Creatinine: 1.1 mg/dL Which medication is most likely contributing to this patient's current presentation?
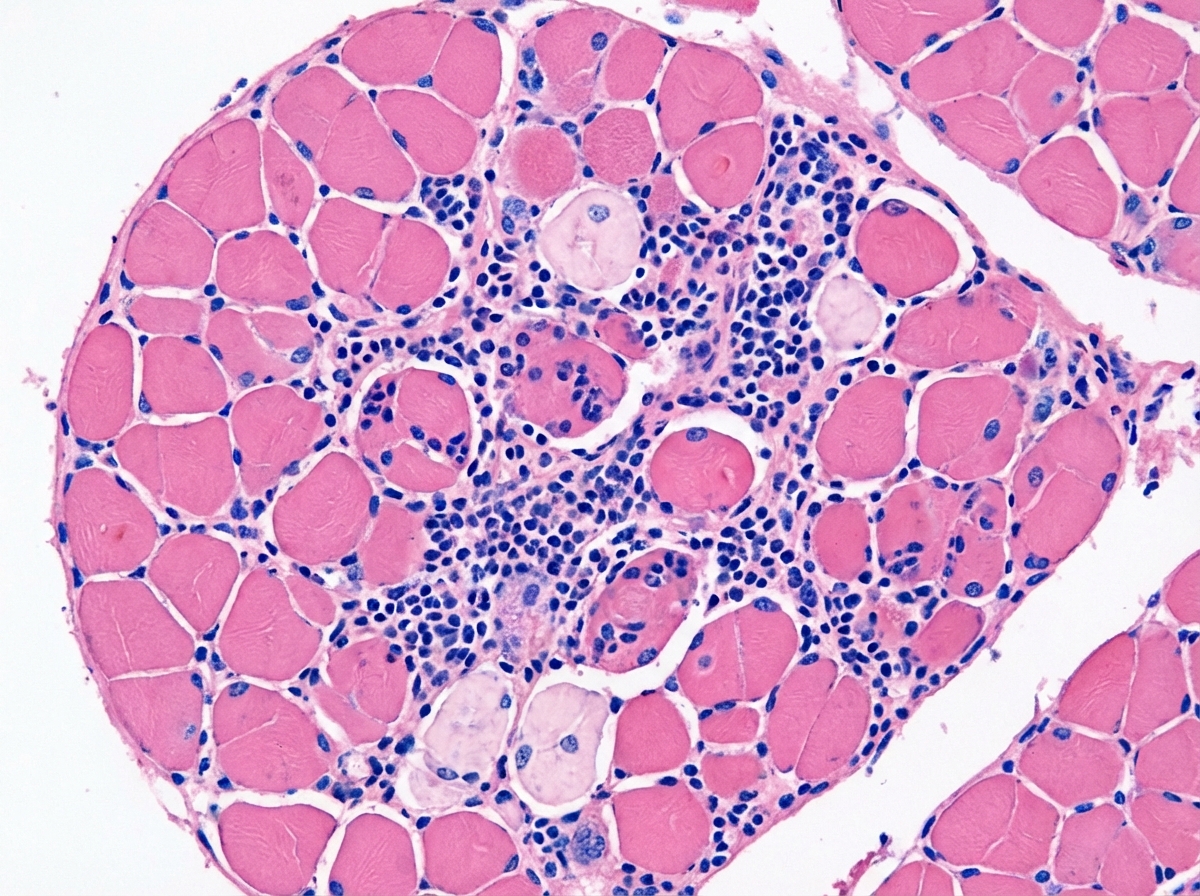
A 26-year-old woman presents with a 3-month history of progressive muscle weakness and dysphagia. She reports choking on her food several times a day but has not experienced aspiration pneumonia, significant weight loss, or airway compromise. She has difficulty climbing the stairs at work. She denies any changes in her routine, diet or muscle pain. Her vital signs include: blood pressure 110/70 mm Hg, pulse 70/min, respiratory rate 13/min, temperature 36.5°C (97.7°F). On physical examination, strength is 3 out of 5 in her upper extremities bilaterally and 2 out of 5 in her lower extremities bilaterally. Laboratory tests are significant for the following: Mean corpuscular volume 92.2 μm3 Erythrocyte sedimentation rate 35 mm/h C-reactive protein 6 mg/dL (ref: 0-10 mg/dL) Anti-citrullinated protein 10 EU (ref: < 20 EU) Creatine kinase (total) 320 U/L (ref: < 200 U/L) Anti-Jo-1 3.2 U (ref: < 1.0 U) Hemoglobin 12.9 g/dL Hematocrit 45.7% Leukocyte count 5500/mm3 Platelet count 200,000/mm3 Differential: Neutrophils 65% Lymphocytes 30% Monocytes 5% Transthoracic echocardiography is unremarkable. A muscle biopsy is performed, and the finding are shown in the exhibit (see image). The patient is started on high doses of systemic corticosteroids, but, after 4 weeks, no clinical improvement is noted. Which of the following is the most appropriate long-term steroid-sparing treatment for this patient?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app