
Autonomic/CV Drugs — MCQs

On this page
A 25-year-old man is brought to the emergency department by his girlfriend for a nosebleed. Pinching the nose for the past hour has not stopped the bleeding. For the past several months, he has had recurring nosebleeds that resolved with pressure. He has no history of hypertension or trauma. He has asthma that is well controlled with an albuterol inhaler. He has intermittent tension headaches for which he takes aspirin. His temperature is 37.9°C (100.2°F), pulse is 114/min, and blood pressure is 160/102 mm Hg. Physical examination shows active bleeding from both nostrils. Pupil size is 6 mm bilaterally in bright light. The lungs are clear to auscultation. The hemoglobin concentration is 13.5 g/dL, prothrombin time is 12 seconds, partial thromboplastin time is 35 seconds, and platelet count is 345,000/mm3. Which of the following is the most likely explanation for this patient's symptoms?
A middle aged man is brought in by emergency medical services after being found unconscious, lying on the street next to an empty bottle of vodka. His past medical history is unknown. Upon evaluation, he opens his eyes spontaneously and is able to obey commands. After peripheral access is obtained, IV normal saline and glucose are administered. Suddenly, the patient becomes confused and agitated. Horizontal nystagmus is noted on exam. This acute presentation was likely caused by a deficiency in which of the following?
A 32-year-old male patient presents to the emergency department after being found down on a sidewalk. He is able to be aroused but seems confused and confabulates extensively during history taking. Physical exam of the eye reveals nystagmus and the patient is unable to complete finger-to-nose or heel-to-shin testing. Chart review shows that the patient is well known for a long history of alcohol abuse. Which of the following substances should be administered prior to giving IV glucose to this patient?
A 64-year-old female with a history of end-stage renal disease presents to her primary care physician complaining of weakness. She reports a six-month history of progressive weakness accompanied by occasional dull aching pain in her arms, legs, and lower back. She has also started to increase her fiber intake because of occasional strained bowel movements. Her past medical history is notable for poorly controlled diabetes, major depressive disorder, and obesity. She takes insulin and sertraline. She has a twenty pack-year smoking history and drinks alcohol socially. Her temperature is 98.5°F (36.9°C), blood pressure is 130/85 mmHg, pulse is 80/min, and respirations are 16/min. Laboratory findings are shown below: Serum: Na+: 138 mEq/L Cl-: 99 mEq/L K+: 3.9 mEq/L HCO3-: 26 mEq/L BUN: 20 mg/dL Glucose: 140 mg/dL Creatinine: 2.0 mg/dL Parathyroid hormone: 720 µU/mL Ca2+: 11.1 mg/dL Phosphorus (inorganic): 4.8 mg/dl A medication with which of the following mechanisms of action is most likely indicated to address this patient’s symptoms?
A 30-year-old man with history of intravenous drug use and methamphetamine-associated chronic thromboembolic pulmonary hypertension (CTEPH) is brought to the emergency department by his girlfriend for worsening abdominal pain and fevers. The patient said the pain was initially around his umbilicus, but he is now experiencing intense tenderness near his groin. He was initially prescribed rivaroxaban, but due to insurance issues, he was switched to warfarin for management of CTEPH two weeks ago. His temperature is 102°F (38.9°C), blood pressure is 95/60 mmHg, pulse is 95/min, respirations are 22/min. He states that his blood pressure usually runs low. His physical exam is notable for an unremarkable cardiac exam, bibasilar crackles, and RLQ tenderness with rebound tenderness when the LLQ is palpated. Laboratory results are shown below: Hemoglobin: 11 g/dL Hematocrit: 35 % Leukocyte count: 16,000/mm^3 with normal differential Platelet count: 190,000/mm^3 Serum: Na+: 137 mEq/L Cl-: 100 mEq/L K+: 3.7 mEq/L HCO3-: 23 mEq/L BUN: 40 mg/dL Glucose: 110 mg/dL Creatinine: 0.8 mg/dL Ca2+: 9.1 mg/dL AST: 34 U/L ALT: 45 U/L International normalized ratio (INR): 6.2 Prothrombin time (PT): 40 seconds Partial thromboplastin time: 70 seconds Blood type: O Rhesus: Positive Antibody screen: Negative A clinical diagnosis is made and supported by the surgical consult team in lieu of imaging. The next operating room for an add-on procedure will not be available for another 5 hours. Appropriate medical therapy is initiated. What is the best next step for surgical optimization?
A 74-year-old female with a history of lung adenocarcinoma status post lobectomy, chronic obstructive pulmonary disease, congestive heart failure, and diabetic nephropathy presents to clinic complaining of hearing loss. Over the last week, she has noticed that she has had difficulty hearing the telephone or the television. When sitting in a quiet room, she also has noticed a high-pitched ringing in her ears. She denies any vertigo or disequilibrium. Further review reveals ongoing dyspnea on exertion and worsening cough productive of whitish sputum for the last month. The patient was recently discharged from the hospital for a congestive heart failure exacerbation. She lives alone and keeps track of all her medications, but admits that sometimes she gets confused. She has a 20 pack-year tobacco history. Her home medications include aspirin, lisinopril, furosemide, short-acting insulin, and a long-acting ß-agonist inhaler. Two weeks ago she completed a course of salvage chemotherapy with docetaxel and cisplatin. Her tympanic membranes are clear and intact with no signs of trauma or impaction. Auditory testing reveals bilateral hearing impairment to a whispered voice. The Weber test is non-lateralizing. Rinne test is unrevealing. Hemoglobin: 11.8 g/dL Leukocyte count: 9,400/mm^3 Platelet count: 450,000/mm^3 Serum (Present visit): Na+: 134 mEq/L K+: 3.8 mEq/L Cl-: 95 mEq/L HCO3-: 30 mEq/L BUN: 45 mg/dL Creatinine: 2.1 mg/dL Serum (1 month ago): Na+: 135 mEq/L K+: 4.6 mEq/L Cl-: 102 mEq/L HCO3-: 24 mEq/L BUN: 22 mg/dL Creatinine: 1.2 mg/dL On follow up visit two weeks later, the patient's hearing has significantly improved. Which of the following is the most likely cause of her initial hearing loss?
A 23-year-old Caucasian male presents to the emergency department with a persistent penile erection for the last 6 hours. He recently began outpatient treatment for depression with associated insomnia. He traveled to Mexico 5 months ago. His medical history is otherwise unremarkable. Which of the following is the most likely precipitating factor for priapism in this patient?
A 42-year-old woman presents to the emergency department with pain in her abdomen. She was eating dinner when her symptoms began. Upon presentation, her symptoms have resolved. She has a past medical history of type II diabetes mellitus, hypertension, heavy menses, morbid obesity, and constipation. Her current medications include atorvastatin, lisinopril, insulin, metformin, aspirin, ibuprofen, and oral contraceptive pills. She has presented to the ED for similar complaints in the past. Her temperature is 98.1°F (36.7°C), blood pressure is 160/97 mmHg, pulse is 84/min, respirations are 15/min, and oxygen saturation is 98% on room air. Physical exam and abdominal exam are unremarkable. The patient is notably obese and weighs 315 pounds. Cardiac and pulmonary exams are within normal limits. Which of the following is the best prophylactic measure for this patient?
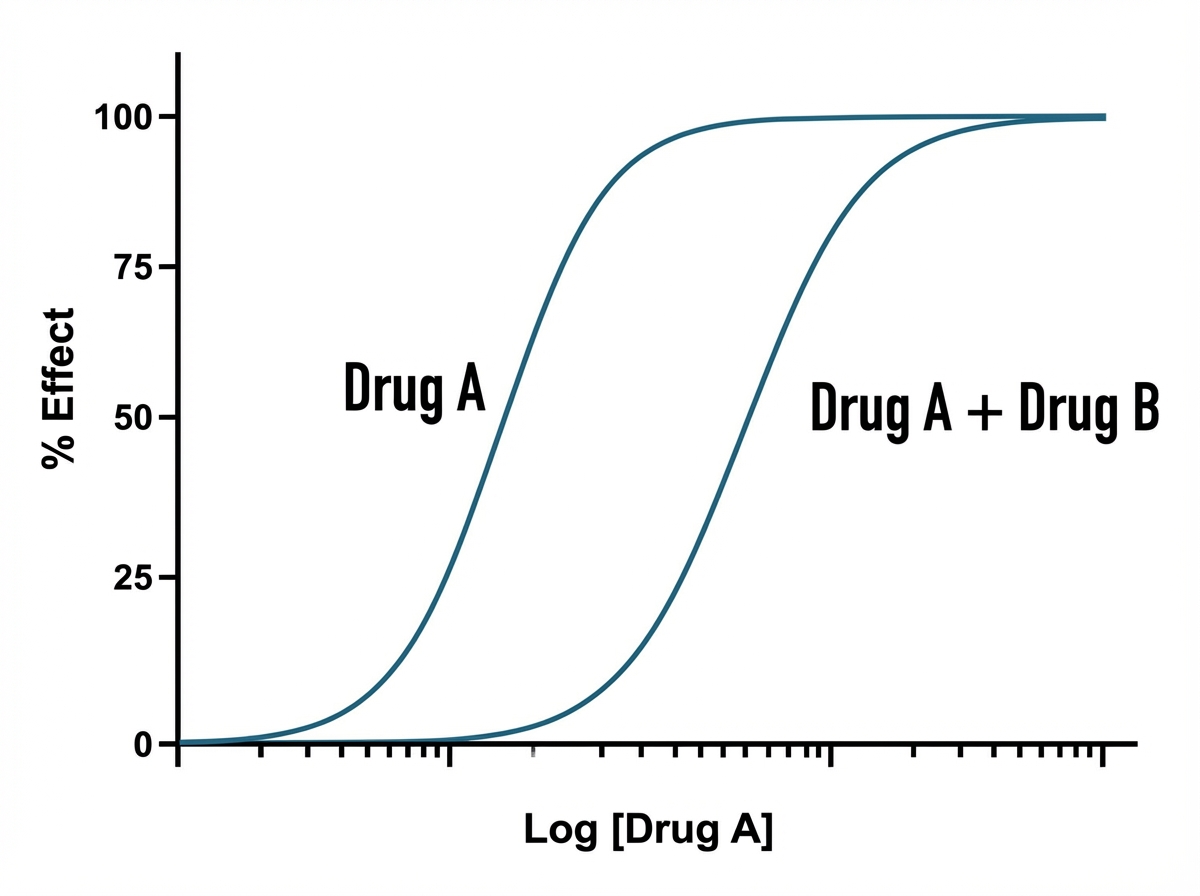
An investigator is studying the interaction between a new drug B and an existing drug A. The results are recorded and plotted on the graph shown. Which of the following properties of drug B best explain the observed effect on the dose-response curve of drug A?
A 3-year-old boy presents with progressive lethargy and confusion over the last 5 days. He lives with his parents in a home that was built in the early 1900s. His parents report that "his tummy has been hurting" for the last 3 weeks and that he is constipated. He eats and drinks normally, but occasionally tries things that are not food. Abdominal exam shows no focal tenderness. Hemoglobin is 8 g/dL and hematocrit is 24%. Venous lead level is 55 ug/dL. Which therapy is most appropriate for this boy's condition?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app