
Autonomic/CV Drugs — MCQs

On this page
A 48-year-old man comes to the emergency department because of a 1-hour history of heavy nasal bleeding. He drinks half a bottle of sherry daily. His pulse is 112/min, and blood pressure is 92/54 mm Hg. Physical examination shows scattered ecchymoses across the extremities and oozing from a venipuncture site. Laboratory studies show a prothrombin time of 28 seconds and a partial thromboplastin time of 36 seconds. Impaired function of which of the following proteins is the most likely cause of this patient's hemorrhage?
A 59-year-old woman is scheduled to undergo a right hip total arthroplasty for severe hip osteoarthritis that has failed conservative management. She has never had surgery before. She has a history of major depressive disorder and takes sertraline daily and ibuprofen occasionally for pain. Her mother died of breast cancer and her father died from a myocardial infarction. She has a brother who had an adverse reaction following anesthesia, but she does not know details of the event. In the operating room, the anesthesiologist administers isoflurane and succinylcholine. Two minutes later, the patient develops hypercarbia and hypertonicity of her bilateral upper and lower extremities. Her temperature is 103.7°F (39.8°C), blood pressure is 155/95 mmHg, pulse is 115/min, and respirations are 20/min. A medication with which of the following mechanisms of action is most strongly indicated for this patient?
A 70-year-old man comes to the physician for the evaluation of pain, cramps, and tingling in his lower extremities over the past 6 months. The patient reports that the symptoms worsen with walking more than two blocks and are completely relieved by rest. Over the past 3 months, his symptoms have not improved despite his participating in supervised exercise therapy. He has type 2 diabetes mellitus. He had smoked one pack of cigarettes daily for the past 50 years, but quit 3 months ago. He does not drink alcohol. His current medications include metformin, atorvastatin, and aspirin. Examination shows loss of hair and decreased skin temperature in the lower legs. Femoral pulses are palpable; pedal pulses are absent. Which of the following is the most appropriate treatment for this patient?
A 4-year-old boy is brought to the emergency department with intense crying and pain in both hands after playing with ice cubes. His mother denies any preceding trauma. The temperature is 37.0°C (98.6°F), the blood pressure is 90/55 mm Hg, and the pulse is 100/min. The physical examination shows swollen dorsa of the hands and scleral icterus. The laboratory tests show hemoglobin of 10.1 g/dL and unconjugated hyperbilirubinemia. The cellulose acetate electrophoresis shows 60% HbS and absence of HbA. Which of the following can reduce the recurrence of the patient’s current condition?
A 21-year-old woman was brought to the emergency department after her roommate found her unconscious at their apartment. On arrival, her GCS was 3/15, with bilateral mydriasis, fever of 39.4℃ (103.0℉), and ventricular tachycardia which was converted to sinus rhythm. She had one episode of a generalized tonic-clonic seizure on the way to the hospital which was managed with intravenous diazepam. Her hypertension was managed with nitroglycerin. After nasogastric tube insertion, gastric lavage and activated charcoal were given. Biochemistry result showed elevated creatine phosphokinase (CPK) of 268 U/L and low serum bicarbonate of 16.7 mmol/L. Her blood and urine samples will most likely show intoxication with which of the following drugs?
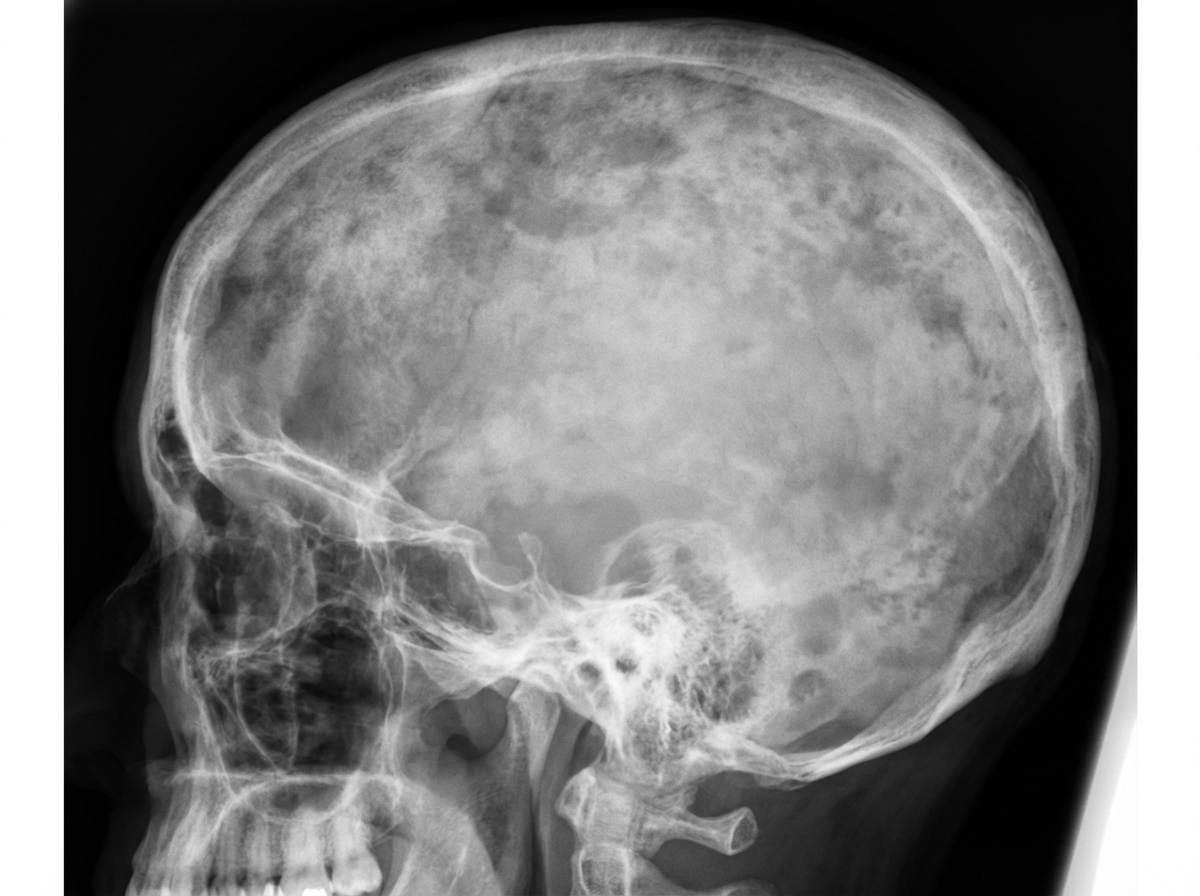
A 58-year-old man comes to the physician because of a 6-month history of headaches and back pain. Examination shows mild sensorineural hearing loss. Serum concentration of alkaline phosphatase is increased. An x-ray of the skull is shown. The most appropriate pharmacotherapy for this patient is a drug that has which of the following mechanisms of action?
A 66-year-old man presents to the emergency department for shortness of breath for the last 2 hours. Despite his diagnosis of heart failure 2 years ago, he has refused to make any diet changes. He takes aspirin and carvedilol but is poorly compliant. His vital signs are pulse of 135/min, respirations 30/min, and a blood pressure of 150/80 mm Hg. The patient is visibly distressed and unable to lie down. He is taking shallow breaths and auscultation reveals bilateral crackles in the chest. Jugular venous distension is seen. Pitting edema is present in the lower limbs. A chest X-ray shows prominent interstitial markings bilaterally with alveolar infiltrates. Which of the following is the mechanism of action of the drug that can relieve his ongoing symptoms?
A 61-year-old man with longstanding diabetes and coronary artery disease presents to the ER with chest pain and dyspnea. The echocardiogram reveals moderate-to-severe mitral regurgitation and an ejection fraction of 27%. A chest X-ray shows bibasilar infiltrates. A new drug is added to his medication regimen, and the physician mentions urinary frequency, increased breast tissue development, and erectile dysfunction as possible side effects. What is the mechanism of action of this drug?
A 32-year-old woman comes to the emergency department because of a 3-hour history of severe nausea, vomiting, tremor, and anxiety. She recently started a new medication but does not remember its name. She has a history of major depressive disorder treated with fluoxetine. Her temperature is 38.9 C (102.1 F), pulse is 132/min, respirations are 22/min, and blood pressure is 152/94 mm Hg. She is confused. Physical examination shows diaphoresis and an ataxic gait. Patellar reflexes are 4+ bilaterally. This patient's condition is most likely due to which of the following medications?
An 8-year-old girl is brought to the physician by her mother because of a 6-month history of an episodic dry cough, shortness of breath, and chest tightness. She has seasonal allergic rhinitis. Physical examination shows high-pitched expiratory wheezes throughout both lung fields. Pulmonary function testing shows an FEV1 of 70% (N ≥ 80%). Which of the following drugs would be most effective at reducing bronchial inflammation in this patient?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app