
Autonomic/CV Drugs — MCQs

On this page
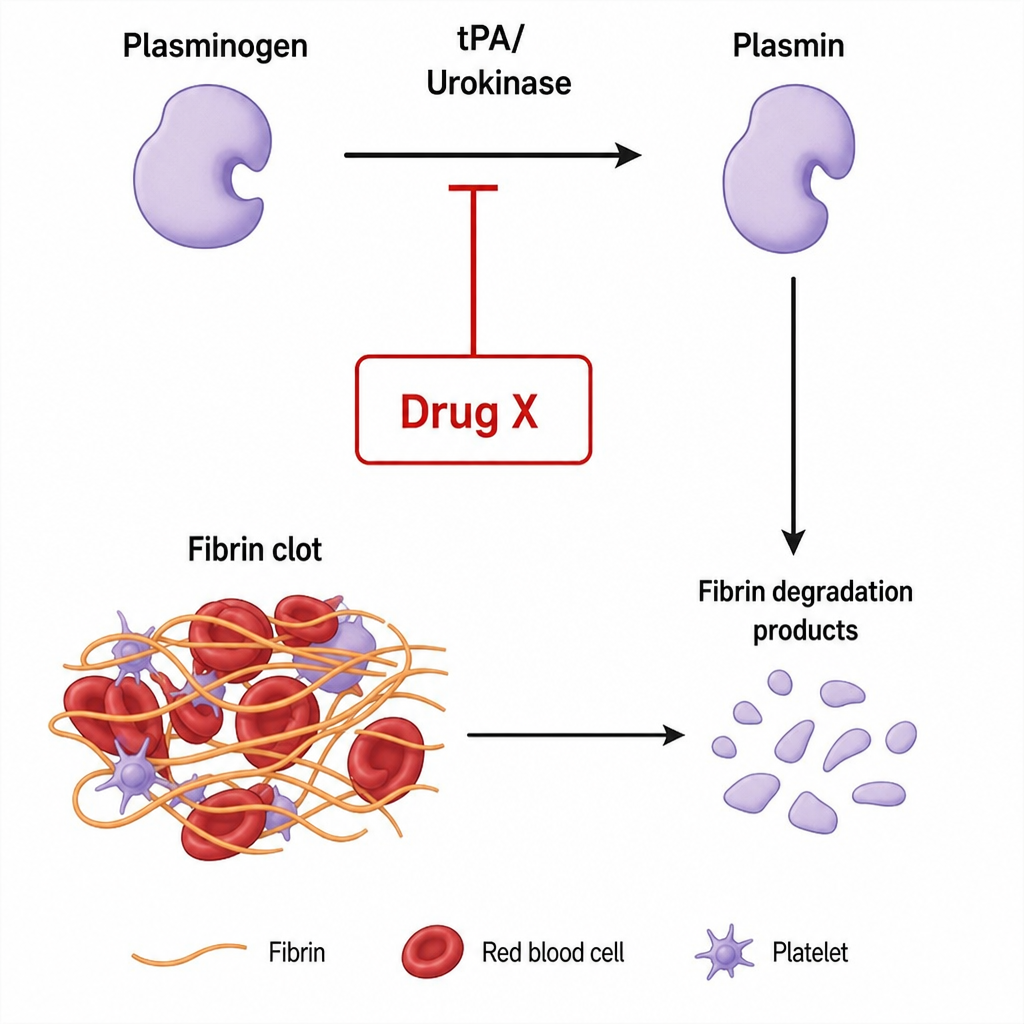
Which of the following is represented in the below figure by drug X?
A patient with a history of binge alcohol intake presented to the emergency department with convulsions, altered sensorium, and a plasma glucose level of $45 \mathrm{mg} / \mathrm{dL}$. Which of the following treatments is needed?
What is a potential consequence of administering indomethacin beyond 36 weeks of gestation?
A 50-year-old patient with renal insufficiency was recently operated on for pyelolithotomy. Which drug is the most appropriate choice for post-operative analgesia?
Which of the following is false about pheochromocytoma?
Which of the following drugs is used for the long term management of obesity
Topiramate is used in
A 19-year-old woman with a history of poorly controlled asthma presents to her pulmonologist for a follow-up visit. She was recently hospitalized for an asthma exacerbation. It is her third hospitalization in the past five years. She currently takes inhaled salmeterol and medium-dose inhaled budesonide. Her past medical history is also notable for psoriasis. She does not smoke and does not drink alcohol. Her temperature is 98.6°F (37°C), blood pressure is 110/65 mmHg, pulse is 75/min, and respirations are 20/min. Physical examination reveals bilateral wheezes that are loudest at the bases. The patient’s physician decides to start the patient on zileuton. Which of the following is the most immediate downstream effect of initiating zileuton?
A 60-year-old man presents to the emergency department for fatigue and feeling off for the past week. He has not had any sick contacts and states that he can’t think of any potential preceding symptoms or occurrence to explain his presentation. The patient has a past medical history of diabetes, hypertension, and congestive heart failure with preserved ejection fraction. His temperature is 98°F (36.7°C), blood pressure is 125/65 mmHg, pulse is 90/min, respirations are 14/min, and oxygen saturation is 100% on room air. Laboratory values are obtained and shown below. Hemoglobin: 12 g/dL Hematocrit: 36% Leukocyte count: 6,500/mm^3 with normal differential Platelet count: 197,000/mm^3 Serum: Na+: 147 mEq/L Cl-: 105 mEq/L K+: 4.1 mEq/L HCO3-: 26 mEq/L BUN: 21 mg/dL Glucose: 100 mg/dL Creatinine: 1.1 mg/dL Ca2+: 10.1 mg/dL AST: 12 U/L ALT: 10 U/L Urine: Appearance: clear Specific gravity: 1.003 The patient is admitted to the floor, a water deprivation test is performed, and his urine studies are repeated yet unchanged. Which of the following is the best next step in management?
A 25-year-old female with a history of childhood asthma presents to clinic complaining of a three month history of frequent, loose stools. She currently has three to four bowel movements per day, and she believes that these episodes have been getting worse and are associated with mild abdominal pain. She also endorses seeing red blood on the toilet tissue. On further questioning, she also endorses occasional palpitations over the past few months. She denies fevers, chills, headache, blurry vision, cough, shortness of breath, wheezing, nausea, or vomiting. She describes her mood as slightly irritable and she has been sleeping poorly. A review of her medical chart reveals a six pound weight loss since her visit six months ago, but she says her appetite has been normal. The patient denies any recent illness or travel. She is a non-smoker. Her only current medication is an oral contraceptive pill. Her temperature is 37°C (98.6°F), pulse is 104/min, blood pressure is 95/65 mmHg, respirations are 16/min, and oxygen saturation is 99% on room air. On physical exam, the physician notes that her thyroid gland appears symmetrically enlarged but is non-tender to palpation. Upon auscultation there is an audible thyroid bruit. Her cranial nerve is normal and ocular exam reveals exophthalmos. Her abdomen is soft and non-tender to palpation. Deep tendon reflexes are 3+ throughout. Lab results are as follows: Serum: Na+: 140 mEq/L K+: 4.1 mEq/L Cl-: 104 mEq/L HCO3-: 26 mEq/L BUN: 18 mg/dL Creatinine 0.9 mg/dL Hemoglobin: 14.0 g/dL Leukocyte count: 7,400/mm^3 Platelet count 450,000/mm^3 TSH & Free T4: pending A pregnancy test is negative. The patient is started on propranolol for symptomatic relief. What is the most likely best next step in management for this patient?
Practice by Chapter
Antiarrhythmic classification and mechanisms
Practice Questions
Class I antiarrhythmics (sodium channel blockers)
Practice Questions
Class II antiarrhythmics (beta blockers)
Practice Questions
Class III antiarrhythmics (potassium channel blockers)
Practice Questions
Class IV antiarrhythmics (calcium channel blockers)
Practice Questions
Other antiarrhythmic agents
Practice Questions
Antianginal drugs
Practice Questions
Positive inotropic agents
Practice Questions
Phosphodiesterase inhibitors
Practice Questions
Cardiac glycosides
Practice Questions
Vasopressors and inotropes
Practice Questions
Pulmonary hypertension therapies
Practice Questions
Peripheral vascular disease therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app